
Health Services Restructuring in Canada
New Evidence and New Directions
Edited by Charles M. Beach, Richard P. Chaykowski, Sam Shortt, France St-Hilaire and Arthur Sweetman
Repeated injections of large amounts of additional money into the health care system allows governments to avoid confronting the most important structural weakness in Canada’s health care system – its lack of incentive to increase productivity.
Improvements in productivity are the key to making the health care delivery system more cost effective and reducing the rate at which health care expenditures grow. In other fields, competition among service providers has been shown to be the best way – indeed, perhaps the only way – to drive improvements in productivity. Thus, the introduction of competition in health care delivery is not an end in itself. It is the means of encouraging improvements in productivity that will lead to a much more efficient and cost-effective delivery system.
Canada’s single-payer system yields considerably more administrative efficiencies than any multifunder arrangement. Most importantly, the single public funder ensures that no one will be denied care due to an inability to pay.
However, the Canadian health care system precludes competition among sellers of health care services. The resulting monopoly occurs at two levels: health care professionals and hospitals. Health care professionals hold monopoly power because they are the sole providers in their respective areas of expertise (doctors, nurses and so on). Hospitals hold monopoly power because they do not compete for patients on the basis of either price or quality of service.
The result of this structure is an imbalance of bargaining power between governments, as funders, and groups of providers. The imbalance stems from two facts. First, health care is an essential service, and governments (and the public) greatly fear strikes in the health care sector. Second, work rules – who does what and under what conditions – are virtually never part of collective bargaining, as they are in other industries.
The excessive power wielded by associations of health care providers has enabled them to win pay increases that have surpassed those achieved in other industries. These increases were secured with virtually no consideration for increases in productivity or variations in the quality of services delivered by different providers.
We do not suggest that reform should be accomplished on the backs of those who deliver health care services. Rather, what concerns us is the structure of a system in which truly essential work (health care) is performed by groups of workers whose monopoly position is not effectively counterbalanced in the course of collective bargaining.
Significant productivity improvements could be achieved by better utilizing providers. Health care professionals should be able to use the full range of their skills and knowledge rather than being limited by rigid scope-of-practice rules.
However, substituting lower-cost (but fully qualified) professionals for more expensive ones is made virtually impossible by scope-of-practice rules that are under the sole control of the various professional associations. In addition, most health care workers have narrow job descriptions that excessively limit the range of tasks they are permitted to do. As a result, hospitals have relatively little flexibility in organizing their services.
The way in which provincial governments fund hospitals also generates inefficiencies. Today, hospitals have little incentive to enhance the quality and/or accessibility of their services, to contain or reduce costs, to improve their efficiency or to improve their productivity. This is largely because their annual budgets are not based directly on the volume and type of procedures performed in a given year, nor do they reflect the actual cost of providing these services. The key question is: How can the system be changed to drive down excess costs and improve productivity in the delivery of health care services?
In a system as complex and multifaceted as health care, a top-down command and control strategy will almost certainly lead to compounding existing inefficiencies. Effective reform can only be achieved by putting in place a set of incentives that encourage individuals and institutions, acting in their own self-interest, to make the changes that are required. In essence, the introduction of what are usually called “market forces” is the only effective way to make the health care delivery system more efficient and its providers more productive.
A key way to encourage competition would be to change from the annual hospital budgeting system to a service-based funding system. This would lead to the establishment of specialized stand-alone facilities (or clinics) that would be able to offer lower prices for procedures such as cataract surgery, some orthopaedic surgeries, diagnostic tests and so on. These facilities would be cheaper to operate because of lower overheads and more flexible job descriptions. As well, greater specialization would lead to improvements in service quality. Finally, competition would encourage hospitals to contract out nonmedical services in order to improve productivity and reduce costs.
Nothing in our proposals for generating competition requires, or even provides an incentive for, the introduction of for-profit delivery facilities. All of the benefits could be achieved regardless of whether service delivery facilities are publicly or privately owned, for-profit or not-for-profit.
Canada’s health care system must not only be preserved, but it must also be made more cost-effective, more efficient and more productive. These results can only be achieved through the introduction of competition into the delivery of health services.
The latest taboo in Canada’s publicly funded health care system is not the creation of a parallel private health care insurance system – this would be unacceptable to a majority of Canadians – but rather the introduction of greater competition within the existing health care delivery system.
Various groups in Canada have been largely successful in asserting – without any supporting argument or evidence – that competition among providers would put Canada on a slippery slope to an American-style system. The irony of this position is that without increased productivity, for which competition provides a powerful incentive, timely access to medically necessary treatment in Canada will be inhibited further. This would, in turn, increase demand for a parallel private for-profit tier of health care services (which would violate the Canada Health Act).
This paper proposes a set of reforms to increase efficiency, reduce waiting times for medically necessary services, and make Canada’s publicly funded, single-payer health care system more productive and financially sustainable. The current habit of governments of promising billions of additional dollars to “cure the problems” of the health care system is neither workable nor financially sustainable over the long term. It is not sustainable because, to date, by adding money, governments (and those within the system) have simply managed to avoid confronting the most important structural weakness of Canada’s existing system: its lack of incentive to increase productivity.
Improvements in productivity are the key to making the health care delivery system more cost-effective and to reducing the rate of growth of health care expenditures. In other fields of endeavour, competition among providers has been shown to be the best way – indeed, perhaps the only way – to drive improvements in productivity. Competition in health care delivery is not an end in itself, but it is a valuable tool – the means of achieving improvements in productivity that will lead to a much more efficient and cost-effective delivery system.
We can achieve competition among providers while preserving the single-payer, publicly funded system and upholding the principles of the Canada Health Act. In its report The Health of Canadians, released in October 2002, the Standing Senate Committee on Social Affairs, Science and Technology strongly supported the single-payer model, both because it assures all Canadians of equitable treatment and because it is the most efficient way to pay for health care services.
In this paper, we explain why improved productivity resulting from competition in the delivery of health care services is essential. In so doing, we outline a number of proposed changes that address current inefficiencies in the provision of health care. These include: implementing service-based funding for hospitals, devolving further responsibility for the purchase of health services to regional health authorities and reviewing the scope-of-practice rules for health care professionals. In addition, we urge that a study of the productivity of various health care providers be undertaken. All these changes were recommended by the Senate committee in its 2002 report.
We believe strongly that the changes we propose are essential. The health care system that is cherished by Canadians is simply not fiscally sustainable without them. We also caution, however, that still more changes may be required if the ones we propose do not sufficiently reduce the rate of health care cost increases. In this sense, our proposals constitute the minimum set of changes required.
Canadian health care is based on a single public insurer for the buying/funding of medically necessary health services (there being but a single buyer is referred to in the economic literature as a “monopsony”). Although there are many providers of health services in Canada, they can be thought of collectively as a monopoly provider because they all operate according to a set of rules and a financing system that effectively preclude their competing with one another. In particular, Canada’s many hospitals and doctors do not compete on the basis of price or quality of service.
The single-public-insurer (buyer/funder) model for health care derives from the public administration criterion of the Canada Health Act, which stipulates that provincial/territorial health care insurance plans must be administered on a not-for-profit basis by a public agency. This model essentially precludes the operation of a parallel private insurance sector in competition with public insurance for the funding of services provided by hospitals and doctors and covered by the Canada Health Act.
That government is the sole participant in the field of insuring medically necessary services provided by hospitals and physicians is often wrongly interpreted to mean that government is also responsible for the delivery of the services it funds. In fact, the delivery of publicly funded health care in Canada currently is almost entirely in the hands of the private sector: most doctors are in private practice (they operate like small businesses or self-employed professionals) and the great majority of hospitals are private nonprofit organizations.
Laboratory and diagnostic services paid for by the single public insurer are provided in most provinces by private for-profit companies. Laundry services, meal preparation and other support or ancillary services in publicly funded hospitals are often delivered by private companies operating on a for-profit basis. Thus, Canada has a mixed public-private delivery system. It is simply not true that the delivery system is public. Nor is it true that the Canada Health Act requires publicly insured services to be provided by public sector institutions or employees.
To repeat, we feel strongly that the single-public-funder system must be preserved. The Senate committee established clearly that the single public insurer for health care yields considerably more administrative efficiencies than any multifunder arrangement. More importantly, a single public funder ensures that no one will be denied necessary care due to an inability to pay. It is this universal feature of the system that is most cherished by Canadians.
The single-payer system is more efficient than multiple-payer models because it covers all Canadians and thus spreads the cost of insuring against ill health across the widest possible pool of people: the entire population. It also eliminates the inequities and inefficiencies related to adverse selection – competing voluntary insurance plans may refuse to insure high-risk patients and/or charge everyone higher premiums to compensate for the fact that more people at higher risk of ill health will buy insurance than people at lower risk (see Banting and Boadway 2004).
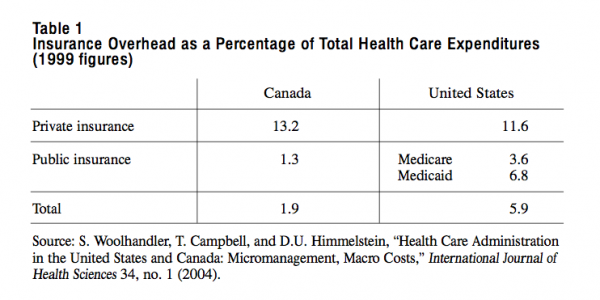
The single-payer system also substantially reduces the administrative cost to hospitals of processing and administering health insurance claims. For example, a 2004 study (using 1999 figures, in US dollars) concluded that the overall administrative costs (including hospitals and doctors’ offices) accounted for 31 percent of total health care expenditures in the US ($1,059 per capita), compared to 16.7 percent in Canada ($307 per capita) (Woolhandler, Campbell and Himmelstein 2004). If its administrative costs were the same as Canada’s, then the United States would save $209 billion per year, more than enough to insure the 40 million Americans who currently have no health insurance.
Examining insurance overhead only, the overhead cost per capita for health care insurance was $259 in the US, compared with $47 in Canada, representing 5.9 percent and 1.9 percent of total health care expenditures, respectively. It is very clear that, in addition to its cherished egalitarian attribute, the single-funder model is also the more administratively efficient by far.
However, while the single-payer model is administratively more efficient, it is also prone to certain systemic problems that can drive up operational costs. Within the publicly funded system, a monopoly situation (in which competition among sellers of health care services is precluded) occurs in the provision of health services at two different levels: health care professionals and hospitals. We will treat each of these separately.
Within each province, associations representing health care professionals hold monopoly power in that each is the sole source of health care providers in its respective area of expertise (doctors, nurses and so on). This, combined with the single-public-insurer model, leads de facto to a bilateral monopoly in which the insurer and provider negotiate uniform province-wide reimbursement rates or salaries.
The outcome of these negotiations depends on the relative power of the bargaining parties. Experience shows, however, that this power is unbalanced: it tends to rest almost entirely with professional associations, in part because of the justifiable fear that governments have of confronting strikes by health care providers, and in part because of major flaws in the existing structure of negotiations.
The imbalance of power between the funder and provider groups stems from the fact that work rules – dictating which employees will do what, and under what conditions – are virtually never part of the negotiations, as they are in other industries. Typically, in the course of negotiations, labour will seek higher wages while management will seek changes to the working environment that will foster greater productivity and lead to a decrease in per unit production costs. These productivity savings are then shared by the employees (through higher wages and benefits) and the employer (through higher profits).
Unfortunately, in health care negotiations, changes to work rules are virtually never negotiated. All that is negotiated are wages or salaries. Thus, that which is crucial to the funder (the government) – how to improve the productivity of the system – is not on the table. All that is subject to bargaining are the issues that potentially benefit the providers – namely, wages/incomes. Therefore, the critical trade-offs involved in balancing wage increases against productivity improvements are not even addressed at the bargaining table, let alone resolved.
In recent years, the excessive power wielded by associations of health care providers has secured pay increases that have surpassed those bargained in other industries. Thus, according to the Conference Board, “during the 1990s, health workers, in general, saw their median annual earnings rise twice as much as non-health workers (6.4 percent versus 3.1 percent) and health professionals experienced a 15.1 percent increase” (Conference Board of Canada 2004, 57). Moreover, these increases have been secured without much, if any, consideration for increases in productivity or differences in the quality of services delivered by individual providers.
This cannot continue. We are not suggesting that reform should be accomplished on the backs of those who deliver health care services. Nor are we suggesting that the ability of various providers to secure the best possible return for their services be unduly restricted. Rather, what concerns us is a situation in which a truly essential service (health care) is provided by groups of workers whose monopoly position is not effectively counterbalanced in the course of their negotiations with government (the single payer) or with employers (for example, hospitals, whose funding is determined almost entirely by the single payer).
Because health care is so labour-intensive, resolving the current imbalance in negotiating power is critical. For example, the minister of health planning in British Columbia estimates that approximately 80 percent of total acute care costs in that province are labour costs. Thus, of the $1.1 billion that was added to BC’s health care budget in 2002, $685 million went to increases in the wages, fees and benefits paid to health care workers.
Elsewhere, professional associations of health care workers have either already secured pay increases significantly greater than inflation or are preparing to take advantage of the infusions of new federal health care funds into provincial treasuries. A few pertinent examples include:
The biggest problem that governments, and hence taxpayers, face as funders of the system is meeting the fee and wage demands of the various groups of health care workers.
As we have said, there is nothing wrong with people using their bargaining power to seek the best possible deal they can get. What is wrong is an arrangement that gives them a lopsided advantage in negotiations. At the heart of the problem is a system that does not permit a proper balance between providers’ desire for wage/salary increases and government’s objective, in its role as funder of the system, of increased productivity.
In addition to retaining a monopoly over the supply of services, professional associations determine the scope-of-practice rules that set out what each type of health professional is allowed to do. Because scope-of-practice rules are the responsibility of the professions, neither they, nor any other work rules, are subject to negotiation with the health system funders. As a result, changes are strongly resisted by anaesthetists, for example, even though nurse-anaesthetists and other professionals are now trained to provide some of the same services just as well and at a lower cost.
There is clear evidence that the Canadian health care system could be made significantly more productive through the better utilization of providers. Much would be accomplished if health care professionals of all kinds were allowed to use their full range of skills and knowledge rather than being limited by rigid scope-of-practice rules.
One apt and often-cited example is that of nurse-practitioners, who remain heavily constrained at present by the scope-of-practice rules of the medical profession. Their case is, however, far from unique: many professionals are limited in what they can do by the scope-of-practice rules that exist for other groups of professionals. In its report, the Senate committee saw this as analogous to calling in an electrician to change a light bulb. Of course the job will be done well, but it will not be done in a cost-effective manner.
But professional scope-of-practice rules are not the only source of organisational constraints that perpetuate inefficiencies in the system. Most health care workers have narrow job descriptions that limit the range of tasks they are permitted to do when they are capable of doing much more. As a result, hospitals, in particular, have relatively little flexibility in the way they organize service delivery.
The combination of unbalanced bargaining power and highly restrictive job descriptions seriously limits the extent to which the productivity of all health care workers can be improved. This is true despite the enormous technological advances made in recent years. Whereas in other industries, technological advances have resulted in remarkably increased productivity and lower cost per unit of service, this has not happened in health care.
By way of illustration, consider cataract operations. When medicare was first introduced in the late 1960s, a cataract operation was a major medical procedure requiring the patient to be hospitalized for an extended period and demanding a considerable amount of the ophthalmologist’s time. Today, thanks to advances in laser and lens implant technology, a cataract operation does not require hospitalization and can be done in a fraction of the time. As the Conference Board puts it, the time-cost of practitioners in this field has been reduced “from a matter of hours to a matter of minutes” (Conference Board 2004, 66). Yet this dramatic increase in productivity has not been reflected in a proportionately lower fee for performing the procedure. Similarly, other productivity increases arising from technological advances, such as in arthroscopic surgery, have not resulted in lower costs to the taxpayer, although they have resulted in higher income for some practitioners.
It is clear that there are significant barriers to cost adjustment in health care services compared with that in other service industries. The issue is therefore how best to remove these barriers and expose health care delivery to the same type of pressures that help generate productivity increases elsewhere. In our view, the introduction of competition among health care providers offers the greatest promise.
The way in which provincial governments fund the hospital component of the delivery system also generates inefficiency. In provinces where they exist, regional health authorities (RHAs) have only partial control over health care spending. For the most part, they receive a budget – in the form of block funding – from the provincial government, which they often simply pass on to hospitals and other care providers based on historical service delivery patterns rather than on the number and type of services actually being provided. That is, the services a hospital actually provides during the year are not taken into account in determining its revenue. Not only are annual budgets not based directly on the volume and type of procedures performed in a given year, but they also fail to reflect the actual cost of providing such services.
Because hospitals and other providers do not have to compete on the basis of either quality or price in order to attract funding, they have little incentive to enhance the quality and/or accessibility of their services, to contain or reduce costs or to improve their efficiency or effectiveness. In others words, there are very few incentives for them to improve their productivity.
Exactly the same situation exists in Ontario, the only province that does not have RHAs. There, health department bureaucrats fund hospitals directly with annual budgets that are based on historical patterns and not on current services provided.
Without competition, the monopoly provider of hospital services drives up costs and constrains productivity gains:
We cannot stress strongly enough that in our view, and in the view of the Senate committee, failure to improve the productivity of health care delivery will result in the system, as it is presently structured, becoming financially unsustainable in the reasonably near future. In its report, the Senate committee concluded that “there are real, continuing upward pressures on Canada’s health care costs” and that, therefore, “Canada’s publicly funded health care system, as it is currently operated, is not fiscally sustainable given current funding levels” (Standing Senate Committee on Social Affairs, Science and Technology 2002, 255). Among the factors that compelled the committee to reach this conclusion were the impact of the aging population, rising drug costs and the need to invest in expensive new technologies.
The Conference Board, in its March 2004 study of health care cost drivers, reached the same conclusion as the committee had two years earlier. For example, it estimated that one-third of projected real health care expenditure growth could be attributed to the aging population. The report stressed that this represented a heavier burden than that imposed by other cost pressures, such as population growth, because, “unlike the other cost pressures aging comes with no offsetting increase in income or wealth that can finance additional cost increases” (Conference Board 2004, 22).
The aging population also compounds the pressures caused by rising prescription drug prices. Public spending on drugs has doubled over the past 20 years; those over 65 years of age accounted for 64.5 percent of all provincial/territorial spending on drugs in 2000 (Conference Board 2004, 36), while representing just over 12 percent of the population. The unending stream of new technologies that expand the capacity of the health care system to serve Canadians is another important source of escalating costs.
In its report, the Senate committee stressed that the “increase in the percentage of government spending devoted to health care provides the clearest indication of the financial pressures felt by governments charged with funding health care” (Standing Senate Committee 2002, 257). In this regard, the Conference Board pointed out that “without structural change in how health care is delivered, the current systems will grow from consuming about 32 percent of total provincial/territorial revenues to 44 percent in 2020” and that “some provinces could spend in excess of 50 percent of their budgets on health care by 2020, just as the demographic bulge of Canadian seniors starts to pass through the systems” (Conference Board 2004, 86). A recent Alberta report indicated that since 1997, provincial health spending has increased by 10.4 percent per year, while provincial revenues have only grown at a rate of about 4 percent per year (MLA Task Force on Health Care Funding and Revenue Generation 2004, 4).
Clearly, compounded year after year, such increases are not sustainable over the longer term. Indeed, some provinces could hit the fiscal brick wall in a very few years. This bleak picture implies that productivity increases are essential if our publicly funded health care system is to survive. Therefore, the key question is: How can the system be changed to eliminate excess costs and improve productivity in delivering health care services?
Typically, in Canada, the problem has been addressed using a top-down command-and-control approach, with health department bureaucrats instructing service providers on what to do. This is the approach embodied, for example, in Ontario’s recently enacted Bill 8, The Commitment to the Future of Medicare Act.
The Senate committee recommended a different approach. It concluded that in a system as complex and multifaceted as the health care system, a top-down command-and-control model would not work – it would almost certainly lead to even greater inefficiency. Effective reform, the committee maintained, could only be achieved by putting in place a set of incentives for individuals and institutions, acting in their own self-interest, to make the required changes. In essence, the committee argued that the introduction of what are usually called “market forces” would be the only effective way to change the health care delivery system, to make it more efficient and to make its providers more productive.
Competition among health care institutions and providers is essential to break the present monopolistic stranglehold of provider groups and to ensure that Canadian taxpayers get full value for every dollar spent on health care. We believe strongly that competition will also lead to the development of new and innovative forms of health care delivery, substantially improving productivity. Furthermore, we believe that competition is in everybody’s best interest – the insurer, the hospital, the physician and other health professionals. Ultimately, though, the patient and taxpayer will benefit the most.
Canada is not the only OECD country struggling with health care costs, as a special supplement to the July 17, 2004 issue of The Economist on health care finance amply illustrates. In particular, The Economist emphasizes that “governments’ attempts to contain health care costs have come in many forms including budget caps, usually in the hospital sector; wage controls; price limits on medical fees and prescription drugs; restrictions on the flow of new medical students; and delays in the introduction of new technologies” (Wallace 2004, 15). All of these have been tried in Canada, and they have failed, just as they have failed in other OECD countries. According to The Economist, “the underlying reason why these methods fail is that they do nothing to provide greater efficiency” (Wallace 2004, 15).
So how would competition in service delivery address the problems of the present system? The government, the insurer (funder), would choose to buy insured services from the lowest-cost provider who meets specified quality conditions. Providing the opportunity for institutions to bid to provide specific services would create an environment in which those patients requiring relatively simple procedures would be drawn away from teaching hospitals to community hospitals, with their lower cost structure. Such competition would force large teaching hospitals to examine closely the spectrum of services they offer and to redefine their roles.
Competition would also lead to the establishment of specialized, stand-alone facilities (or clinics) able to offer the lowest price for procedures such as cataract operations, some orthopaedic surgeries, various diagnostic tests and hernia repair. Not only would such specialized facilities, concentrating on a limited range of procedures, be less expensive, but they would also be expected to achieve better results as a consequence of higher volumes. In medicine, the more frequently the same procedure is performed, the higher the quality of the outcomes. Thus, specialized facilities would both reduce costs and improve quality. (In fact, some experts have suggested that the waiting time for cataract operations could be eliminated within a year if all such operations were done in specialized clinics instead of hospitals.)
With respect to reducing costs, the smaller the institution, the more flexible the job descriptions of its various staff members. Greater flexibility in utilizing human resources is a very compelling factor in support of specialized health care clinics. Efficiencies and productivity improvements could also be gained if people were encouraged to rely on 24-hour community clinics for many of the primary care services they currently receive in hospital emergency rooms.
Competition would encourage hospitals to contract out nonmedical services in order to improve productivity and reduce costs. Using a tendering process, hospitals would procure these services from the lowest-cost provider, subject only to the provider’s meeting appropriate and closely monitored quality standards.
Such changes in the delivery system would, in turn, prompt all service providers to find ways to improve the quality and cost-effectiveness of their services in order to avoid losing work to more cost-effective institutions or providers. In this way, reform of the system would occur gradually, driven by incentives rather than by the top-down, command-and-control approach that has been so clearly demonstrated to be ineffective.
It is important to note that all the benefits described here could be achieved regardless of whether service delivery facilities are publicly or privately owned, forprofit or not-for-profit. Nothing in our proposals for generating competition in health services delivery requires, or even provides an incentive for, the introduction of for-profit delivery facilities. Publicly owned institutions can compete with one another, just as privately owned institutions do in any competitive marketplace. Therefore, our proposals do not depend in any way on the specific ownership structure of the health care delivery system. In this regard, we should note that in its report the Senate committee argued that government, as the insurer (funder) of the system, should be indifferent as to who owns a service delivery institution and on what basis it operates as long as comparably high-quality outcomes are achieved by the organizations and institutions offering services at the lowest price.
Since the inception of Canada’s national health care program, the role of government has been as a funder, not a provider, of health care. As the Senate committee documents in its report, one of the great myths about Canada’s “public” heath care system is that it includes public delivery as well as public funding. This has never been the case. Beginning with hospital insurance in 1957 and continuing with the creation of medicare in 1966 and the enactment of the Canada Health Act in 1984, the central objective has always been to insure Canadians against hospital and doctor costs and improve their access to medically necessary health care services. No legislation restricts the ownership of health care institutions.
Therefore, it is difficult to understand the rationale for the recent decisions by the Manitoba NDP government to purchase a for-profit orthopaedic clinic in Winnipeg and by the Ontario Liberal government to purchase three for-profit MRI clinics in the province as well as to require four others to convert to not-for-profit status. First, it is important to recognize that these institutions are different from the MRI clinics that exist in Quebec. These take private-pay patients who can then jump the queue in the publicly funded system and are thus clearly part of a parallel, privately funded tier of health care. More importantly, purchasing the facilities in Manitoba and Ontario simply means that money will have been taken out of cash-strapped health care budgets and spent in a way that provides no added benefits to patients and does nothing to shorten a single waiting line.
Moreover, past experience indicates that public ownership of these facilities will not ease the burden of the rigid work rules of publicly owned hospitals described earlier in this paper and of the higher salary scales of public institutions as compared to clinics. Thus, not only will capital funds have to be spent with no patient benefit, but also the resulting higher operating costs will further deplete health care budgets.
In addition, moving these facilities to the public sector will strengthen the monopoly bargaining position of the health care workers involved. As we have explained, this is precisely the wrong direction for public policy to move in if our objective is to make the health care system financially sustainable.
In order to introduce competition to the institutional health care delivery system and enhance its productivity, we must change the way in which hospitals are funded. The Senate committee recommended that hospitals employ service-based funding. That is, hospitals should be paid an agreed-upon fee for each service they deliver after that service has been performed. It is the change from global budgets to this funding mechanism that makes possible the competitive market described earlier.
Again, such funding changes are not unique to Canada. As The Economist points out, “One building block [of a more efficient health care system] is the introduction of prospective payment systems for hospital services [essentially, what the Senate report calls ”˜service-based funding’]. For example, Australia, Sweden, Britain and Germany are moving this way and hope to have the new payment system up and running within four years” (Wallace 2004, 18).
We recognize that a service-based funding system will not work in all circumstances. It will work in urban community hospitals, but teaching hospitals, as well as rural or remote hospitals, should be treated differently because it is not possible to create a market for many of the services they provide. For example, because many of the sophisticated procedures that they alone can perform require highly specialized equipment and personnel, teaching hospitals cannot be funded solely through a service-based funding system. Service-based funding should be used only for the more common procedures performed in both teaching hospitals and community hospitals.
In addition to their role as service provider, academic health science centres play major roles in teaching and research. The Senate committee recommended that these roles be financed with base funding, which would be separate from the funding for their clinical service role.
Once fully established, the incentives built into service-based funding would generate a number of significant benefits. They would:
A specific and highly desirable benefit of service-based funding would be its ability to demonstrate clearly to the public the relative efficiencies of hospitals offering comparable services. Because hospitals would be competing with each other to serve patients, the inefficient hospitals would either lose business (because the price they bid would be too high), or they would lose money (because they were unable to perform the service at the price they bid). The Economist article echoes this conclusion, noting that prospective payment (or service-based funding) systems are “likely to do some good…because they show us the poor performers and create pressures on the hospitals to become more efficient” (Wallace 2004, 18).
Looked at in this light, whether a hospital made a profit (or a surplus, in the case of those operating on a not-for-profit basis) or showed a loss/deficit in a year would be a true reflection of the effectiveness of its management and provider team and of the efficiency with which it operated. But under the current global budgeting model, whether a hospital makes or loses money in a given year depends principally on how good provincial health department bureaucrats are at estimating the volume and mix of the procedures the hospital carried out during that year and, to a substantial degree, on what that hospital did in the past. This is hardly an accurate reflection of the competence of hospital managers. Nor is it an effective way to make hospital CEOs more accountable.
Finally, a benefit of service-based funding that should not be underestimated is its psychological impact on people employed in hospitals. Under service-based funding, a patient coming into a hospital would be important not only as a person in need of help but also as a source of revenue; that person could no longer be considered a drain on the hospital’s limited resources as determined by its global budget.
The rigid entrenchment of scope-of-practice rules and their regulation by the relevant professional associations has resulted in the inefficient use of scarce human resources in health care. These rules prevent many health care professionals from providing the full range of services they have been trained and are qualified to provide in cases where there is a conflict with another health profession’s scope-of-practice rules. Such rules can also severely impede multidisciplinary collaboration, particularly in primary health care.
Critically important is the fact that rigid scope-of-practice rules drive up health care costs. The most highly educated and skilled professionals spend inordinate amounts of time on matters that could just as easily be handled by other fully qualified providers with less training. This is costly to the system as a whole and makes for less satisfying work for the overqualified professionals.
Scope-of-practice rules must be revised to allow all categories of health care professionals to practise to the full extent of their capacities. This revision would:
We know very little about the factors that influence productivity in health care and how the productivity of key personnel in the system can be improved. We do know, however, that the explosion of new knowledge and major advances in technology have increased the productivity of other professions over the past 20 years. Surely, better diagnostic equipment, more effective drugs, improved out-of-hospital treatments, better-educated and better-trained nurses, counsellors, rehabilitation therapists, pharmacists and physicians, combined with the improved health status of Canadians, have made health care professionals more productive. Yet this has not been reflected in the cost of providing health care services.
An assessment of the productivity of the various health care professions must be undertaken. Such an assessment should include a review of the barriers to productivity gains. Without the removal of these barriers, health care costs will continue to escalate at a fiscally unsustainable rate. Information on productivity in health care will help to:
During the last decade, Canadian RHAs have done a commendable job of organizing health services for people in their regions. We believe that they offer great potential to foster competition among hospitals and other health care providers. If they are to do so, however, they must be given more responsibility and greater authority for delivering and/or contracting for the full range of publicly insured services. The devolution of such responsibility from provincial governments to RHAs, making them exclusive purchasers of services, would complement the introduction of service-based funding.
RHAs would buy health services on behalf of the patients they serve, contracting with the hospital, clinic or nonmedical provider that provides the best level of service: the best combination of service quality, timely delivery and price. The devolution of the purchasing function from provincial governments to RHAs could then be extended to other providers, including specialist physicians, primary health care physicians and testing laboratories (see Jérôme-Forget and Forget 1998). This would:
It is important to stress that by encouraging the fostering of competition at the regional level we are not implying that the public hospitals currently owned by RHAs should be turned over to the private sector. Competitive contracts could be awarded by the RHAs to public hospitals, but the competition would be enhanced if private providers were allowed to compete with the public providers for at least some publicly insured health services (such as day surgery). The greater the number and variety of competing institutions, the greater the likelihood of increased efficiency of operation and productivity.
A key element of successful competition among providers – whether public, private, not-for-profit or for-profit – is the requirement that all types of institutions meet uniform, rigorous standards of quality, particularly of outcomes, to ensure that patients receive safe and high-quality care, no matter where or by whom it is delivered.
The incentives we propose to encourage competition in health care can be introduced without threatening, in any way, the single-public-insurer model of Canadian health care or any of the principles of the Canada Health Act. Nevertheless, as we said at the outset, some will argue that these proposals would put Canada’s health care system on a slippery slope to destruction. This is simply not true.
The debate about competition in health care is marked by confusion over the difference between the funding of health care and the delivery of health care services. The advantages of equity and cost-effectiveness associated with having a single public insurer do not apply to the delivery of health care. It is this lack of a clear distinction between funding and delivery in the public debate on health care that has led to the impression that because the single public/government insurer is good, private delivery must be bad. In fact, as we have seen, delivery has been almost entirely in the hands of the private sector since the founding of medicare. Thus, to claim that the private delivery of health services threatens the integrity of the single public insurer is manifestly false, given the actual structure of Canada’s publicly funded health care system.
The Canada Health Act, through its public administration principle, requires a single public insurer for medically necessary hospital and doctors’ services and, therefore, excludes experimentation with private financing for these services. The Act, however, does not address the issue of the ownership structure of health care delivery institutions. It does not require that such institutions be either public or not-for-profit, nor does it prevent a province or RHA from contracting out the delivery of publicly funded services to private providers operating either on a not-for-profit or for-profit basis. Simply put, if services are fully publicly insured, then the participation of private, for-profit providers (physicians, laboratories, hospitals, other health care facilities and so on) does not contravene the principles of the Canada Health Act or the values that underpin it.
The introduction of competition, in and of itself, would not favour the private sector in any way. The corporate structure of the competing entities providing services under our proposed framework would be irrelevant, just as it is now irrelevant under the Canada Health Act. All health care facilities, no matter their ownership and basis of operation, would be subject to a common, rigorous and independent quality control and evaluation process to ensure their accountability.
Perhaps the weakest link in Canada’s health care system is its failure to hold accountable in any effective way those who manage or fund the system. Not only should all health care providers be subject to uniform standards of service quality, but they should also be accountable for the public funding they receive. It is equally important that the insurers (governments) themselves be accountable to those who elected them and to the people who rely on them to organize the delivery of health services efficiently.
If we are to have a health care system that truly serves Canadians, both governments and providers must become much more accountable to those whom the system should serve: the people – as patients, as family members of patients and as taxpayers. Enhanced accountability on the part of all health care players is essential if we are to improve productivity and thereby sustain publicly funded health care.
The measures put in place to discharge greater accountability, however, must function with as little bureaucracy as possible. Provincial governments have tried various mechanisms to hold hospital boards and CEOs accountable for their performances. While their objective of improved accountability is sound, the usual means of trying to achieve it – top-down control by provincial bureaucrats of highly complex service delivery institutions – are not effective. Nothing as complex as a hospital can ever be managed from afar.
Accountability, with a minimum of bureaucracy, requires two things: first, an independent body with the means and ability to monitor the performances of governments and health care providers; and, second, appropriate incentives to obtain the desired results. With regard to the first requirement, we are pleased to note that there is considerable agreement that the newly formed National Health Council should be responsible for reporting to Canadians on the performance of the health care system.
But this is not enough. Accountability cannot be based entirely on periodic reports or press releases, important as these are. Decisions, made daily, that expedite or impede access to high-quality care crucially affect the health of patients in need and the well-being of their families. Accountability for such decisions requires much more immediate and meaningful mechanisms. Strong incentives must be introduced – positive ones that reward good performance and negative ones that have teeth to punish poor performance.
The central objective of our publicly funded health care system must be to ensure that Canadians have timely access to the high-quality care they need, and that those responsible for funding and delivering the care are held accountable for meeting that goal. As it is currently constituted, our system allows governments and providers to shift the consequences of excessive waiting times onto the backs of patients and their families – sadly, at present, doing so costs governments and providers little or nothing.
This is why it was easy for governments to cut back on health care funding during the 1990s without first implementing the changes that would allow the system to achieve greater productivity. They closed hospital beds and reduced the number of doctors and nurses being trained. What they did not do was simultaneously increase the number of substantially less expensive home- and community-based beds for those who did not need hospital care. Nor did they tackle scope-of-practice rules so as to permit nurse-practitioners, nurses, counsellors and other health professionals to provide, to the full extent of their competencies, an expanded range of health care services. Public dissatisfaction with Canada’s publicly funded health care system spiked during this period, as government spending cuts took their toll on those waiting for care.
We believe that a system of incentives is required that will place the burden of meeting acceptable standards of care on those who are actually responsible for funding, organizing and delivering that care. In the view of the Senate committee, the core of such a system must be a formal, binding guarantee to Canadians that they will get the care they need, when they need it. This does not mean that Canadians should be entitled to instant service. Clearly, some rationing of the supply of health care services occurs in every health care system. The issue is: When does the rationing become excessive? Or, as it emerged in early June 2004, when the Chaoulli case went before the Supreme Court of Canada: When does the rationing of the supply of health care services become so severe that a patient’s Charter rights are violated? (Dr. Jacques Chaoulli and a patient asked the court to overturn two Quebec court judgments that upheld provincial laws limiting the use of private medical services or medical insurance; they maintained that their Charter rights were breached by these laws.)
That is the reason why the Senate committee recommended the implementation of a health care guarantee that would oblige governments to provide care within reasonable, clinically based waiting times. Of course, such a guarantee would not entitle patients to receive immediate service. This is how the Senate committee put it in its report:
The point at which this health care guarantee would apply for each procedure would be based on an assessment of when a patient’s health or quality of life is at risk of deteriorating significantly as a result of further waiting. Waiting times would be established by scientific bodies using clinical, evidence-based criteria…In keeping with its philosophy that the best way to reform a complex system such as health care delivery is to introduce appropriate incentives for all the players involved, the Committee is firmly convinced that governments must be made to bear the responsibility for their decisions. Thus, the Committee believes that the blame for the waiting list problem should be placed where it belongs – on the shoulders of governments for not funding the system adequately, and jointly on governments and providers of health services, the providers for not developing clinical, needs-based waiting list management systems and governments for not demanding and funding such systems to ensure the rationality of waiting lists, including those that are attributable to underfunding. The Committee believes that governments must pay for the remedy, namely patient treatment in another jurisdiction, while waiting list management systems are being developed and put in place. (Standing Senate Committee 2002, 118, 117)
The bite of this guarantee lies in the requirement that governments pay for treatment wherever it is available (including outside the country), should the maximum waiting time be exceeded and a patient’s health be in danger of deteriorating. Governments must incur a penalty – the cost of sending the patient for treatment in another jurisdiction – for their excessively tight rationing of health care services to deter them from continuing to download the consequences of waiting onto patients. Thus, the health care guarantee is to government what competition is to health service providers – namely, the incentive for appropriate changes in behaviour (see Courchene 2003).
The effect of such a guarantee would be to make governments (and, indirectly, providers) responsible, on a day-to-day basis, for ensuring that patients get the care that they need in a timely fashion. Governments would be forced to ask themselves if they wanted to send a patient outside the country for treatment when the requisite care could be provided at home at a lower cost.
It is because we believe so strongly in making governments accountable for waiting times that we, along with our colleagues on the Senate committee, recently intervened in the Chaoulli case before the Supreme Court. We hoped that the Court might reach the same conclusion that the committee had reached in its report:
[G]overnments can no longer have it both ways – they cannot fail to provide timely access to medically necessary care in the publicly funded health care system and, at the same time, prevent Canadians from acquiring those services through private means…[The committee] passionately hopes that it will not be necessary for…a parallel system of private delivery, financed by private insurance, to emerge…The Committee…categorically rejects the status quo: Canadians in need of medically necessary services must be given timely access to them. (Standing Senate Committee 2002, 120-21).
Critics of the health care guarantee, including Roy Romanow, have suggested that it is not a practical proposal, and that it will therefore create public expectations that cannot be fulfilled. We believe that it is both practical and realistic to set clinically determined maximum waiting times for all major procedures and key diagnostic tests. The Canadian Medical Association and the Canadian Orthopaedic Association have supported this position, most recently in their joint intervention in the Chaoulli case before the Supreme Court.
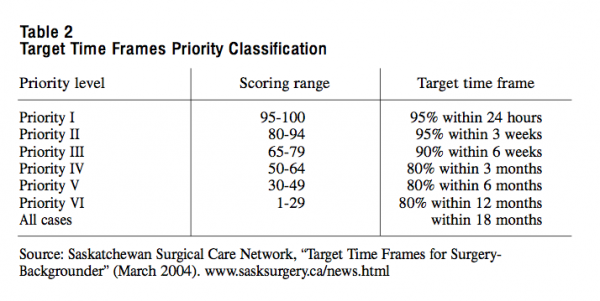
Moreover, we think that the surgical-waiting-time guidelines that were recently introduced by the province of Saskatchewan are a further indication of the practicality of implementing a health care guarantee. As of March 2004, the province has begun to implement the country’s first comprehensive system to rate and track all patients waiting for surgery. The key difference between the Saskatchewan system and the committee’s proposal for a care guarantee is that the wait times that are posted in Saskatchewan represent performance targets rather than an enforceable commitment.
Under the Saskatchewan system, physicians assess patients using a common set of criteria. Individual scores are based on a patient’s condition and the type of surgery required. The patient is placed on one of six priority levels, each having a “target time frame” indicating how quickly he or she should have surgery (as illustrated in the following table). The target time frames apply to all surgical specialties and procedures and were developed by the Saskatchewan Surgical Care Network (SSCN) and its surgical services subcommittee, in consultation with doctors and specialists.
What the health care guarantee would do is convert such waiting-time guidelines into legally enforceable maximum-waiting-time limits. From statements of good intention, these guidelines would become legally enforceable service standards. If it is feasible to establish guidelines, then it is only the absence of political will that blocks their conversion into a maximum-waiting-time guarantee.
Canada’s health care system, with its unique single-public-insurer model, must not only be preserved but also made more cost-effective, more efficient and more productive. We believe that these results can only be achieved through the introduction of competition into the delivery of health services in the ways we have described. We conclude, however, on a cautionary note. As we observed in the opening section of this paper, if the changes we propose fail to yield the desired increases in productivity and the corresponding reduction in the rate of growth of health care costs, then even more changes may be necessary. In a system as complex as health care, one cannot know in advance the full impact of any particular reform. However, we can be certain that the journey down the road to reform must begin with the measures we have outlined in this paper.
Banting, Keith, and Robin Boadway. 2004. “Defining the Sharing Community: The Federal Role in Health Care.” In Money, Politics and Health Care: Reconstructing the Federal-Provincial Partnership, edited by Harvey Lazar and France St-Hilaire. Montreal: IRPP.
Conference Board of Canada. 2004. Understanding Health Care Cost Drivers and Escalators. Ottawa: Conference Board of Canada, March.
Courchene, Thomas J. 2003. “Medicare as a Moral Enterprise: The Romanow and Kirby Perspectives.” Policy Matters 4, no.1. Montreal: IRPP.
Jérôme-Forget, Monique, and Claude E. Forget. 1998. Who Is the Master? A Blueprint for Canadian Health Care Reform. Montreal: IRPP.
MLA Task Force on Health Care Funding and Revenue Generation. 2004. Report of the MLA Task Force on Health Care Funding and Revenue Generation, June.
Standing Senate Committee on Social Affairs, Science and Technology. 2002. Recommendations for Reform. Vol. 6, The Health of Canadians – The Federal Role. Ottawa: Queen’s Printer for Canada, October.
Wallace, Paul. 2004. “The Health of Nations: A Survey of Health-Care Finance.” The Economist, July 17.
Woolhandler, Steffie, Terry Campbell, and David U. Himmelstein. 2004. “Health Care Administration in the United States and Canada: Micromanagement, Macro Costs.” International Journal of Health Sciences 34, no. 1.
This publication was produced under the direction of France St-Hilaire, vice-president, research, IRPP. The manuscript was copy-edited by Mary Williams, proofreading was by Timothy Niedermann, production was by Chantal Létourneau and printing was by Impressions Graphiques.
Copyright belongs to IRPP. To order or request permission to reprint, contact:
IRPP
1470 Peel Street, Suite 200
Montreal, Quebec H3A 1T1
Telephone: 514-985-2461
Fax: 514-985-2559
E-mail: irpp@nullirpp.org
All Policy Matters and Choices are available at irpp.org
To cite this document:
Kirby, Michael J.L., and Wilbert Keon. 2004. “Why Competition Is Essential in the Delivery of Publicly Funded Health Care Services.” Policy Matters 5, no. 8. Montreal: Institute for Research on Public Policy.
Senator Michael J. L. Kirby was the chair of the Standing Senate Committee on Social Affairs, Science and Technology when it released The Health of Canadians, a major study on the state of health care in Canada in October 2002. Senator Kirby has a B.Sc. and an M.A. in mathematics from Dalhousie University. In 1965, he received a Ph.D. in applied mathematics from Northwestern University. Senator Kirby was principal assistant to the premier of Nova Scotia from 1970 to 1973 and served as assistant principal secretary to the prime minister from 1974 to 1976. From 1980 to 1982, Senator Kirby was secretary to the Cabinet for federalprovincial relations and deputy clerk of the Privy Council. In this capacity, he was deeply involved in the negotiations that led to the patriation of the Canadian Constitution and the inclusion of the Charter of Rights in the Constitution. Senator Kirby is a recognized national expert on public policy issues. He served as an advisor to several governments and has held or holds senior directorships on some of Canada’s leading corporate boards. Since his appointment to the Senate in 1984, he has led a number of important inquiries into the banking industry and, more recently, the health care system. He was president of the Institute for Research on Public Policy (IRPP) from 1977 to 1980.
Dr. Wilbert Keon moved to Ottawa in 1969, after his medical and scientific training at the universities of Ottawa, McGill, Toronto and Harvard, to found the University of Ottawa Heart Institute, where he was the president and CEO until April 2004. He also served as professor in and chairman of the Department of Surgery at the University of Ottawa’s Faculty of Medicine for 15 years (1976-91), where the endowed Keon Chair of Surgery has been established in his honour. Dr. Keon has sustained a leadership role in the surgical, academic and scientific community throughout his career. He has held appointments in and elected offices in 36 national and international professional associations and he is a former president of the Canadian Cardiovascular Society and past vice-president of the Medical Research Council of Canada. Dr. Keon is a prolific author with 33 books and 206 research papers and a tireless contributor to academic science as well as well known advocate for health care reform in Canada. Dr. Keon remains active in health and economic policy through his participation on scientific and clinical advisory boards, membership on several boards of directors, as a consultant to public and private sector clients, and as Senator in the Senate of Canada. Senator Keon was also a member of the Standing Senate Committee on Social Affairs.


