
Health Services Restructuring in Canada
New Evidence and New Directions
Edited by Charles M. Beach, Richard P. Chaykowski, Sam Shortt, France St-Hilaire and Arthur Sweetman
The state of Canada’s health care system and the best options for its reform in the face of new challenges have been subjects of debate for well over 10 years. Like the health-care systems of other OECD countries, Canada’s regime faces the growing pressures of fiscal and budgetary constraints while grappling with changing consumer demand, technological innovation and the influence of the private sector. There have been claims of a crisis in the funding, delivery and quality of health services, ample media coverage of critical shortcomings, and the publication of a raft of studies advocating a restructuring of Medicare, all seeking to improve and safeguard the sustainability of the system in the face of growing demand.
Discussions aimed at finding the best model for Canadian health care require a careful approach. This paper proposes a framework for discussion of the future of Canada’s Medicare program and related health and social services informed by the experiences of other jurisdictions while including a healthy recognition of the need for political tenability. The weighing of reform proposals of the health system must take into account not only the gravity of the system’s shortcomings, but also the availability of politically, economically and socially feasible alternatives. This paper examines the reforms to health-care governance implemented by other members of the Organisation for Economic Co-operation and Development (OECD) such as the United Kingdom, France, the Netherlands and Germany, most notably concerning funding and delivery issues. It then analyzes proposals for Canadian health reform, and goes on to discuss proposals to extend Medicare coverage to home care and pharmaceuticals.
The author first argues that such important issues cannot be settled through the use of rhetorical “persuasive definitions” and that policy cannot be guided solely by the invocation of principles. Agreement in principle does not provide guidance for action. The underlying principles of the Canada Health Act are expressions of public support for collective arrangements in health care, but they do not mention what payment form for providers will work best, or what range of services should be included in public health insurance. The governance debate offers insight into the basic requirements for legitimate and effective administration, but does not offer guidance for the actual mix of public and private roles in the funding and delivery of health care. Exploration of that issue requires a knowledge of country-specific characteristics in the social policy arena.
Second, she addresses the issue of cross-border learning. As the experiences of different countries (and those of Canada’s provinces and territories) in developing a variety of administrative arrangements demonstrate, there is more than one way to achieve universal access to services. Though modern industrial states share underlying principles of solidarity and universal access to state-sponsored welfare, they vary in their policy-making and governance styles, reflecting national cultural, political and institutional differences. International experience shows that that there is no universal “best model” of public and private care. What is feasible in one country may be politically or socially untenable in another.
While simplistic pleas for wholesale substitutions of the current model and easy assumptions about the transferability of ideas or social programs should be avoided, Canada can learn from policy experience abroad and from the experiences of its own provinces and territories. Still, there are not many windows of opportunity for the top-to-bottom restructuring of the current system since such arrangements are often resistant to change. Given the country-specific policy context, the opportunities for governments to implement major changes in social policy, such as extending Medicare entitlements to home care and prescription drugs, are rather restricted. What is thus required is a modest and somewhat pragmatic view of the scope of health-care reform.
What is the best public-private model for Canadian health care? This question has been central to many of the health reform debates of the 1990s. Indeed, several recent expert committees claim that the Canadian health-care system is in need of complete restructuring. At first glance, there is much evidence to support that position. There have been many claims of crisis in funding, delivery and quality of health services, and ample media coverage of critical shortcomings. Several reports advocate a restructuring of Canada’s Medicare program in order to improve and safeguard the sustainability of the system in the face of growing demand. For instance, the Mazankowski Report observes that “…without fundamental changes in how we pay for health services, the current system will not be sustainable.”1 Still others conclude that, while adjustments are necessary, the current system is not on the brink of collapse.
A careful analysis of the underlying assumptions, evidence to support certain claims and an ability to draw inferences from such evidence are required to answer this question. It assumes that a study of experiences in other jurisdictions will lead to a better model of funding and delivery of health care, and that such a “better model” will be applicable to the Canadian situation. Whether the problems observed by journalists, academics and policy analysts can be resolved by nothing short of a complete overhaul is a matter of not only assessing the gravity of the shortcomings, but also the availability of politically, economically and socially feasible alternatives. Much of the growing body of literature on cross-country comparison presents a descriptive portrait of experience abroad without attending to the transferability of ideas and policy models.2 It is not easy to draw lessons from mere descriptions of cross-border experience, what is feasible in one country may not be feasible in another.3 What amounts to the best solution in one jurisdiction may be politically or socially unacceptable in another. Given the country-specific historical, cultural and institutional factors that shape social policies, it is hardly surprising that major structural reforms rarely occur. “Windows of opportunity” for wholesale reform seldom present themselves.
The issue of finding the best model for Canadian health care therefore calls for a careful approach to the discussion of health-care reform, starting with detailed mapping of the issues. Only in this way can conclusions about the Canadian situation be drawn.
This paper proposes a framework for discussion of the future of Canada’s Medicare program and related health and social services. In evaluating healthcare funding and delivery issues, the paper uses various public policy models to frame the processes and scope of change. The paper examines the efforts of other member states of the Organization for Economic Co-operation and Development (OECD) to restructure health-care governance, analyzes proposals for Canadian health reform, and uses the conclusions to discuss proposals for extending the Medicare program to cover home care and pharmaceuticals.
The paper opens with a section on the role of government in the development of the modern welfare state. It compares the Canadian experience to that of other industrialized nations. In examining the concept of “governance,” it notes that the term migrated from government to the private sector in the 1970s and 1980s, then back to the realm of public administration in the early 1990s. Interestingly, in the process the term took on a different meaning.
The second section reviews the experience of other OECD member states. Modern welfare states share a number of underlying principles on social policy but have developed a variety of administrative models for the funding, contracting and delivery of health care. These “governance models” also determine the distribution of decision-making powers and financial risks.
The third section focuses on Canada. It begins with a summary of current social policies and the Canadian health-care system, with its distinctive mix of public funding and private delivery, and its regionally administered health insurance. Like other industrialized nations, Canada took decades to develop its current model. Starting in the 1920s with provincial efforts to improve access to a limited range of health-care services, Medicare gradually expanded to a countrywide insurance scheme administered by the provinces and territories. Like other OECD countries, Canada did not escape pressure to change its health-care system. The current arrangements for the funding and provision of home care and pharmaceuticals will then be reviewed, along with recent proposals for healthcare reform.
Next, in assessing health reform proposals of the last decade, the paper raises the issue of “cross-border learning,” the process by which countries seek to learn from experience abroad. While the paper warns against simplistic pleas for wholesale substitution of the current model and against easy assumptions about the transferability of ideas or social programs (including the use of jargon and misleading “persuasive definitions”), it concludes that Canada can learn from policy experience abroad and also from its own experience across provinces and territories.
Finally, we return to the central question of the paper — What is the best model for Canada’s health-care system? — and conclude that the question needs reframing. There is no universal “best model” of public and private care. Nor are there many windows of opportunity for the wholesale restructuring of the current system. International experience shows that existing social arrangements have created their own constituencies and have become resistant to change. Given the country-specific policy context, the opportunities for administrations to implement major changes in social policy, such as extending Medicare entitlements to home care and drugs, are rather restricted. More importantly, agreement in principle does not provide guidance for action. For example, while the underlying principles of the Canada Health Act are expressions of public support for collective arrangements in health care, they do not tell us what payment form for providers will work best, or what range of services should be included in public health insurance. In the face of such restraints and caveats, the question becomes “What policy options will be acceptable to the main stakeholders, given the general agreement on the need for change and the political will to effect change?”
Until the 20th century, services such as income support and health care remained largely in the private realm, provided by families, communities, religious groups and charities.4 Governments played a very modest role.5 After centuries of collective support provided by private actors, the second half of the 20th century witnessed the systematic development of state-sponsored welfare. In the decades after the Second World War, modern welfare states developed a full range of income-protection schemes, health insurance, old age pensions, disability and unemployment benefits, child support and other social services. The scope of the coverage in terms of both risks and populations was extended everywhere, reflecting the growing acceptance of a dominant role for government in sponsoring and providing social services.6 Income-protection schemes replaced earlier forms of mutual support and charity for income loss due to disability, sickness, old age or unemployment on the part of low-income breadwinners and for the support of large families.
In most countries there is strong popular support for the principles of solidarity and equality of access (most visibly in health care). However, the actual sponsorship, funding and administration of services vary across countries and are subject to change. In fact, there is no ultimate model of the welfare state. Rather, the welfare state can be seen as a widely supported collection of underlying principles, with large variance in approaches and implementation.
The institutional histories of modern welfare states have affected policy styles. For instance, the centralist models of the United Kingdom and France contrast sharply with the functionally decentralized models of Germany, Belgium and the Netherlands. These latter models bear the label of neo-corporatism, a type of decision-making whereby governments and private actors (represented through their peak organizations) share responsibility for the shaping and outcome of social policies.7 Neo-corporatism implies that private actors are willing and able to participate in the policy process and to engage in self-regulation. The representative peak organizations of German and Dutch hospitals and physicians represent their members in regional or countrywide negotiations with the health insurance agencies over tariffs and volume of their services; medical associations are empowered to regulate access to their profession, to set standards for medical education and professional conduct, and to police the conduct of all medical professionals (members and non-members alike) with rules and sanctions. The main administrative bodies of health insurance, the sickness funds, are legally independent actors, and their peak organizations have the collective bargaining power to contract health services on behalf of their insured. In some Western European countries, a large share (in the Netherlands, the largest share) of health facilities have always been privately owned and managed (thus not run directly by the state). This is also the case in Canada.
The variations in policy styles and governance might be more easily understood by looking at some of the sociological categorizations developed for modern welfare states. Esping-Andersen identifies three models of the modern welfare state: (a) the “liberal welfare state,” with frugal levels of income protection and targeted services; (b) the “social democratic state,” with high levels of income protection and tight central control; and (c) the “functionally decentralized consensual, corporatist state.”8 This much-quoted typology refers to ideal forms of the welfare state — or, rather, idealized principles. In reality, there are no “pure” models. Most industrialized nations combine elements of at least two of the three models. For example, Canada’s disability and unemployment benefits are frugal compared with those of other countries, based as they are on liberal welfare principles, whereas its health-insurance system has more features of the Western European social democratic systems, with extensive consultation and decentralized administration.
In a decade-old typology of policy styles, Douglas and Wildavsky identify three “dominant cultural orientations” in welfare states: “competitive individualism,” “hierarchical collectivism” and “sectarianism.”9 They do not argue that states belong to one category only. The social democratic states of northern Europe are based on principles of solidarity and equality and have a tradition of collectivism, with moderate individualism and weak sectarianism. They also have a strong bureaucratic tradition. The United States, in contrast, is a liberal welfare state, with weak collectivism and a streak of sectarianism. Market efficiency and individual liberty are its guiding principles. At the same time, the US Medicare and Medicaid health insurance schemes, as well as specific arrangements for veterans and other groups, reflect broad popular support for the protection of “deserving” populations. Canada shares some of the US characteristics but seeks to soften the effects of market competition by promoting solidarity and “good governance” as its guiding principles.
The grouping of countries into broad categories masks important differences among them. For example, the German corporatist model limits the role of the state in social policies such as those for housing and health care. Most if not all organized interests meet with the government for an annual round of negotiations, the “Concerted Action” or Konzertierte Aktion, to set spending levels and the broad allocation of health-care funds. The regional representatives of health insurers and providers then negotiate detailed and binding contracts on the volumes and pricing of health services. Moreover, the federal government has shifted many of the responsibilities for implementing its social policies to the provinces, or Länder.
The Netherlands has copied many of the characteristics of the German model. Until the 1980s the Dutch system was “a striking model of corporatist arrangements,” with private agencies invested with public authority.10 These institutions were not only set up along functional lines, but based on religious denominations. After mounting criticism of this “consociational corporatist” model in the 1970s and 1980s, successive Dutch governments took steps to alter it.11 While Germany and Belgium kept most of their corporatist structures intact, the Netherlands eliminated the direct representation of organized stakeholders in shaping social policies, in an effort to streamline and speed up decision-making. By the end of the 1990s the main interest groups had lost their representation on advisory and administrative bodies. But remarkably, this did not result into a more controversial and conflictuous style of policy negotiations between stakeholders and government. In contrast to the decentralized policy model, France and the United Kingdom have maintained their tradition of centralized power. Under the French étatisme, interest groups have not developed a strong participatory role in social policy. French medical associations are fragmented and show little inclination to collaborate with each other or with government. In contrast, the British Medical Association has played a dominant role in health policies. In the 1940s it accepted the formation of the National Health Service (NHS), which effectively nationalized most hospitals, and in the late 1990s saw the establishment of primary care groups, which effectively altered the self-employed economic status of general practitioners. In exchange, general practitioners have kept their professional autonomy and gained strong influence in the management of health-care institutions.12
The present welfare arrangements in Western Europe and North America can be seen as political systems in the process of continuous development and adjustment. One can argue that the modern welfare state is a collection of principles rather than one distinct model.13 Experience shows that while the basic structures of current welfare arrangements are robust in the longer term, they are subject to gradual change and adjustment. There is no reason to assume that they have reached their “final stage.” The evolution of public and private governance reflects changing ideologies, views and perceptions about the proper role of government and other actors.
In the 1970s private business came under attack from some quarters for its role in society. Accused of racial bias, environmental degradation and gender discrimination, multinational and national corporations began to reconsider their role. Examples of such pressure include the extended protests against the role of Shell in South Africa, legal charges against IBM and other large companies for racial discrimination, the activism of Greenpeace and other environmental groups, and gender battles over access to the boardroom. Other issues drawing media attention were alleged child labour (by subsidiaries and suppliers of Ikea), alleged forced labour (of prisoners in China producing Nike tennis shoes), and alleged fraud and abuse within large corporations. Critics pointed out that a corporation has many stakeholders besides its management, board and shareholders. They also claimed that managing a business is a matter of not only maximizing profits, but also of environmental preservation and social justice. In the 1980s these debates changed the climate of private business. Multinational corporations turned their attention to proper conduct of their business. Their annual reports began to contain policy statements expressing concern about such matters. The Conference Board of Canada framed six guiding principles for the behaviour of the boards of large corporations.15
Business reports use the term “corporate governance” to indicate a broader perspective in the operation of private firms, accepting the principle of accountability to external stakeholders as well as to shareholders. These reports claim that the implementation of such policies requires an entirely new form of internal management, starting with the framing of explicit business goals, measures of success, transparency principles and external reporting new accounting practices are also required.
The governance debate has also taken on an international dimension, with multilateral agencies joining in. In 1998 the OECD issued Principles for Corporate Governance. The privatization unit of the World Bank addresses issues around the private governance of public services. In the 1990s attention was focused not only on corporations but also on the international bodies themselves: the World Bank, the International Monetary Fund and the World Trade Organization (WTO). The annual meetings of these organizations have become the meeting ground for a wide range of protest groups. Critics argue that, increasingly, the debates around important issues of trade, the environment and international development take place behind closed doors, escaping democratic control.16
In the early 1990s the term governance migrated back to government and shed the adjective corporate, taking on good instead. In Britain, the 1992 report of the Cadbury Committee and the 1994 report of the Chartered Institute of Public Finance and Accountancy concluded that the general principles and practices of corporate governance apply to government agencies as well.17 By implication, they also apply to non-profit organizations that provide public goods and services. The above reports frame guidelines for the administration and accounting practices of public agencies, based on the practice of good governance. They argue that in order to be accountable to stakeholders, agencies have to explicitly state their policy goals, means and results. They have to take into account not only the interests of their own personnel and clientele, but also the interests of a wide range of outside parties affected by their operations.
Interestingly, in the process of migrating from the public to the private sector and back again, the term governance lost its neutral meaning. It became what Marmor labels a “persuasive definition” or “aspirational definition,” which means that its very wording suggests either a positive or a negative connotation.18
The same migration from private business (corporate governance) to public administration (good governance) occurred in health care, as business and accounting terms entered that domain.19 There are many examples of the migration of ideas.20 The current wave of enthusiasm for “renewing governments” is framed in terms of the modern business practice.21 Only a few years ago, governments and public agencies (including not-for-profit health-care agencies) were blissfully ignorant of the need to frame an explicit vision or corporate statement. Nowadays, they cannot survive without doing so. They have to frame their “core business” and objectives, redesign their activities in order to increase transparency and accountability, separate their administrative and supervisory functions, and introduce modern bookkeeping methods for improved measuring, monitoring and control. This process of the “creeping corporatization” of health care is visible at all levels of the health-care system.22
In its 2000 World Health Report, the World Health Organization (WHO) introduces the concept of “stewardship” as a measure of the effectiveness of a health-care system. Saltman and Ferousier-Davies argue for the need to “realign the configuration and application of state authority in the health care sector in the interest of achieving agreed policy goals.”23 The concept of stewardship, they claim, “offers the appropriate basis for reconfiguration.” It can “channel emerging systems of integrated care in more socially responsible directions” and, further, “combine efficient market like behaviour with trust based and ethical forms of decision-making, [and] market-oriented reforms with an ethically-driven policy making framework.” These authors define good governance as a desire for policy-making that serves the public interest. Yet while claiming that stewardship offers the promise of improving policy outcomes, they admit that there is no current example of such “ethically informed” or “good” governance — “no country presents a satisfactory operating example of the principles of stewardship” — adding that it will be hard to find people who fit such a role. The WHO report touches upon important issues of governing the delivery of public goods and services. However, replacing current arrangements with an untested and rather abstract model of stewardship will solve nothing.
In the stewardship model, in fact, a new bureaucratic elite, the stewards, would represent citizen and consumer interests in health care. The WHO report serves to illustrate that there is no easy answer to governance questions.
The discussion of the administration of public programs (governance) illustrates the growing influence of the private sector in public policy. It also reveals that certain terms migrate from the private to the public sector and vice versa, losing their meaning in the process. Moreover, the governance debate demonstrates that weighty issues cannot be settled through the use of “persuasive definitions” and that policy cannot be guided through the invocation of principles. The governance debate offers insight into the basic requirements for legitimate and effective administration, whether public or private, but does not offer guidance for the actual mix of public and private roles in the funding and delivery of health care. Exploration of that issue requires a knowledge of country-specific characteristics in the social policy arena.
All OECD countries show strong public support for solidarity-based access to health care for certain population groups (e.g., the elderly, war veterans) or for the entire population. At the same time, public policies, administrative arrangements and stakeholder representation (in particular consumer representation) are reflective of each country’s cultural and institutional legacy, dominant cultural orientation and welfare principles.
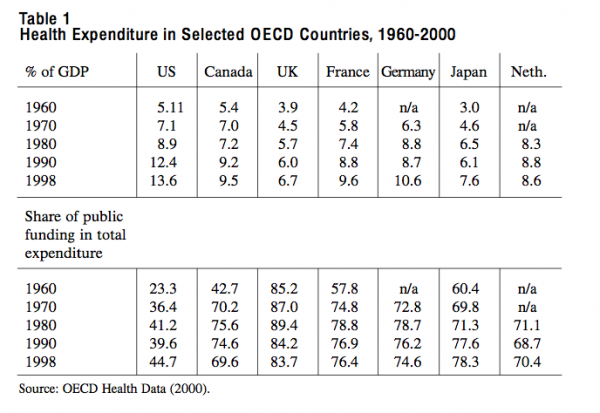
There are also large variations in levels and growth rates of health spending, and in the share of public expenditure going to health (Table 1). In the last four decades, growth rates converged. Between 1960 and 1980 all countries saw a sharp rise in their health spending (measured as percentage of gross domestic product). Thereafter, growth rates levelled off, and in the second half of the 1990s the share of GDP spent on health care even dropped in some cases. Between 1960 and 1990 all countries increased their share of public expenditure on health, although on different levels. The United States was the outlier, with a much lower share of public expenditure. After 1990, the growth of the proportion of public spending stagnated. Except in the United States and the Netherlands, it went down in all countries, most notably in Canada.24
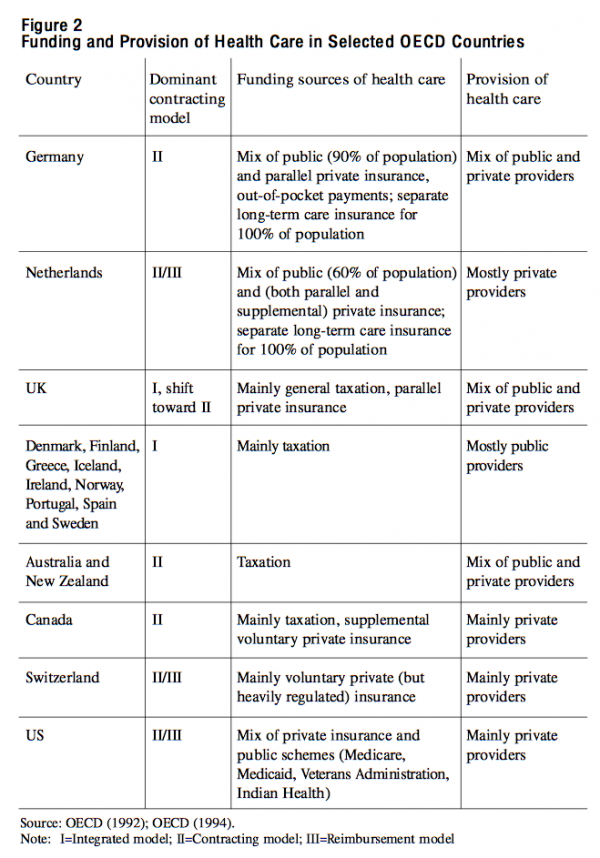
In health care, most if not all OECD countries have embraced the principles of universal and equal access to high quality services. Many have also accepted the right of patients to freely choose their provider and the right of physicians to professional autonomy.25 As the largest proportion of health care is publicly funded, cost-control is an acknowledged goal. Moreover, implicitly or explicitly, most countries see health promotion and consumer safety as important policy goals. The OECD argues that any given health-care system can be characterized by its particular combination of funding and contracting models. In most OECD countries, public funding sources — general taxation, earmarked taxation and social health insurance — predominate, followed by out-of-pocket payments and private insurance. On the contracting side, the OECD identifies three models. In the “integrated model” (Model I in Figure 2), such as the British NHS, the government both funds and provides health care. In the “contracting model” (II), public third-party payers negotiate contracts with independent providers. In the “reimbursement model” (III), which is characteristic of private insurance, patients usually pay the health-care providers and then submit their bills to the health insurers. The OECD concludes that the contracting model, which combines public funding with independent and often private provision of care, is on the rise.
In spite of broad support for the principles of solidarity and universal access, the health-care systems of OECD nations differ greatly in their organizational and governance styles. Health care is provided by a range of ownership and management entities ranging from for-profit firms to religious and other charitable not-for-profit institutions to local or regional authorities. Some arrangements cater for specific population groups while others offer universal access.
Germany was the first country to introduce compulsory health insurance for low-income industrial workers (1883). Denmark followed suit within a decade. Slowly, over the course of many decades, other European countries developed mandatory social insurance schemes covering the risks of disability, sickness, old age and death. France, Belgium and the Netherlands (as well as Japan and Korea) imported the “Bismarckian” model from Germany, with employment-related health insurance. In this decentralized model, legally independent and semi-autonomous sick funds administer social health insurance and negotiate contracts with providers. Other countries sought to extend coverage beyond the working class and introduced population-wide schemes funded out of general taxation, following the example of the British NHS of 1948. In the United States, Germany and the Netherlands, access to social insurance is still limited to specific population groups. The United States has a separate scheme for veterans and also an Indian Health Services. Besides its universal Medicare insurance, Canada has arrangements for veterans and armed forces personnel, prison inmates and First Nations populations. Belgium and France (and also Japan) have extended the sickness-fund model to the entire population. By the late 1990s, the main funding sources for health care in Europe and North America were general (earmarked) taxation and health insurance, both public and private.26
In the Scandinavian countries local and regional authorities have primary responsibility for the funding and delivery of all health and social services. They bear the financial burden of acute medical and nursing care, and have developed extensive social services including home care, support for adjusted housing for elderly and handicapped persons, and support for independent living. In the United Kingdom there is a clear split between the medical care covered by the NHS and the social services provided by local authorities. The Netherlands (1968), Germany (1992) and Japan (1995) have introduced a separate population-wide social insurance to cover long-term care and home care for their aging populations. In all three countries, long-term care insurance is a supplement to their schemes for acute medical care.27 They all feature a mix of public and private providers in this field, and are experimenting with cash benefits allowing consumers to directly contract with providers of care. The above examples show that countries have chosen quite divergent pathways to the goal of universal access to services.
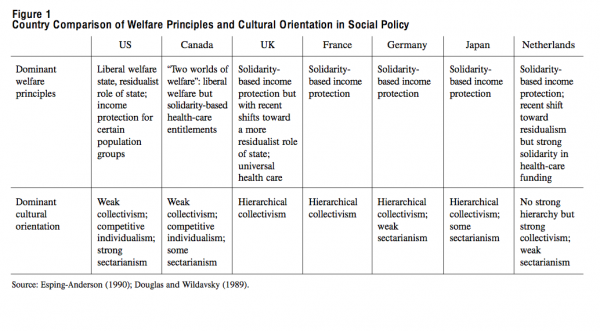
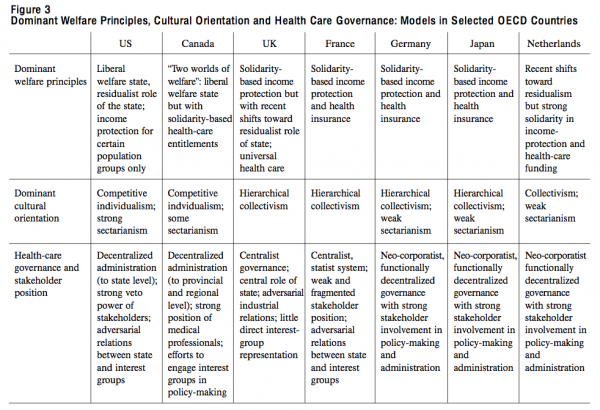
OECD member countries have developed a variety of health governance models. Figure 3 summarizes the social and health policies of selected countries. It combines an overview of dominant welfare principles and cultural orientations with health-care governance models. The scheme shows the diverging “worlds of welfare” in the United States and Canada. The two countries share some dominant welfare principles but have developed very different health-care arrangements. Canada combines elements of the liberal welfare state in macroeconomic and social policies with collectivist and solidarity-based health-care arrangements. The other welfare states exhibit a strong sense of solidarity and acceptance of a dominant role for government, but have developed diverging arrangements for the actual administration and provision of services.
The extent of universal coverage reflects dominant welfare principles, but, with the exception of the United States, all OECD countries provide universal access to health insurance and health-care services through a mix of public and private funding. To a large extent, the funding model determines the governance model: in Western European countries with social health insurance as the main funding source, trade unions and employers’ associations are heavily involved in administering the system. In contrast, in countries with general (federal and/or provincial) taxation as the main funding source, those groups play only an indirect role. In general, neo-corporatist systems, in which interest groups play the dominant role in health policy, feature less conflict among stakeholders than systems in which the state plays the dominant role. In all countries, medical professionals enjoy a strong position.
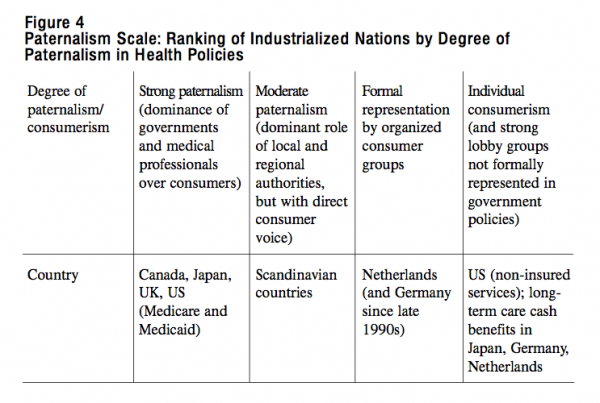
Finally, there is great diversity in consumer representation, a topic warranting special attention in the Canadian health reform debate. The health policies of most OECD countries reflect a high degree of paternalism. The assumption is that governments and medical professionals represent consumer interests in health care, based partly on the characteristics of demand and supply in the health sector. Medical professionals act as agents for patients because of “information asymmetry.”28 Moreover, the largest patient groups — comprising mainly elderly, mentally ill and handicapped citizens — often lack the power to influence social policy. In some countries, specific categories of patients have developed strong and vocal organizations but their existence raises issues of balanced representation and legitimacy. The core question is: To what extent do these individuals speak on behalf of the groups they represent and to whom are they accountable for their views and positions?
This paternalism, which is characterized by representation by bureaucrats and professionals, offers little opportunity for the consumer to have a voice (though patients can, in some cases, choose their own provider or health insurer). It differs markedly from the dominant ideology of consumerism in the United States (though, in actual practice, US consumers have little choice) and the formal representation by organized consumers in Germany and the Netherlands. It is also at odds with growing pressure from dissatisfied consumers and elderly people with sufficient money to purchase the services of their choice; this tension is of particular interest in the current debate on home care.
Figure 4 ranks countries on a “paternalism scale,” ranging from a high degree of (governmental and professional) paternalism to a high degree of consumerism. As with any effort to categorize, the scale does not fully apply to entire systems. However, it does illustrate important differences in the representation of consumer interests. The scale indicates the extent of direct consumer influence in the shaping of health policies and individual decision-making on health-care issues.
For different reasons, both home care and pharmaceutical care drew increasing attention in the 1990s not just in Canada (see page 31) but also in other OECD countries. Since populations are aging, the demand for home care has grown. And since the incomes of elderly populations have also risen, that demand is expressed in both public and private arrangements. The elderly are more educated, self-assured and explicit in their needs and wants today than they were two or three generations ago. Moreover, with the introduction of state-sponsored old-age pensions and with income-related pension schemes, accumulated wealth and savings, today’s elderly generation have money to spend — and are showing a growing willingness to spend it — on home adaptation and additional support services.29 At the same time, governments realize that not all elderly persons can afford to purchase the services they need. They see the expansion of collective home-care arrangements as a desirable and cost-effective substitute for institutional care. Thus home care is at the intersection of private markets and public policies. Existing arrangements reveal a mix of underlying welfare principles, with private payments, means-tested support and universal health-insurance entitlements. In the 1990s several OECD countries engaged in debate over the “best” mix of public and private funding and provision of home care. Germany and Japan extended their social insurance system to include separate universal long-term care insurance. The Netherlands had already introduced such a scheme in the 1960s. This move reflects a growing recognition that home care is a social risk requiring financial pooling rather than an individual risk. In fact, it is remarkable that in a decade of retrenchment two major industrial nations have extended the range of their welfare arrangements.
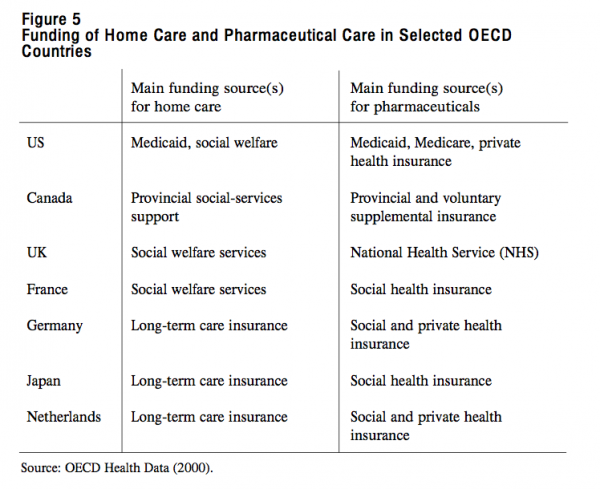
While drugs expenditures in most OECD countries are still relatively modest, their share grew rapidly in the 1990s.30 Hence pharmaceutical care has risen on the political agenda, with concerns being raised about financial barriers for the population groups most in need of drugs such as the elderly and the chronically ill. In most OECD countries with social health insurance and tax-based systems, pharmaceuticals are included in entitlements. However, neither Canada nor the United States have universal entitlements for drugs. Both the US Medicare scheme and Canada’s Medicare cover only drugs that are prescribed in hospitals. In Canada, the provinces have developed a variety of supplemental insurance schemes for the elderly and some other population groups (see also page 35). In most OECD countries, patients face the burden of co-payments for pharmaceuticals prescribed outside of hospitals and other institutions. Figure 5 shows the variety of arrangements for home care and pharmaceutical care in selected countries.
In the mid-1970s the expanding role of the state came under mounting attack. The oil crisis brought economic stagnation and persistently high levels of unemployment. Revised demographic projections revealed a rapidly aging society. A change in ideological views of the state and the individual challenged the authority of church, state and other institutions. Left-wing critics objected to the growing intrusion of the state in private life.31 Right-wing politicians advocated more individual liberty and financial responsibility.32 The two sides came together in challenging the dominant role of the state.
The confluence of these ideological, demographic and economic factors, combined with rising fiscal deficits caused by increased public spending and a levelling off of tax revenues, gave rise to extended discussion on the future of the welfare state. The terms and tone of the debate changed. The welfare state came under attack. It was seen not as the solution to problems caused by industrialization, but as the cause of problems.33 Government was no longer viewed as the ideal representative of the interests of citizens. Critics focused on the inefficiency of government and its the failure to deliver on social policy. They charged that the state had come to replace too many of the responsibilities of individuals and the private sector. Ronald Reagan’s “let’s get government off our backs” became the conservative war cry. Rodrik compares this shift in thinking to the “swing of a pendulum, from one set of ideas which give primacy to the role of the government over markets to another stressing the advantages of markets over the government — and then back again.”34
After decades of expansion, welfare arrangements started to contract. Several countries engaged in extensive debate on the future of the welfare state. The golden era of expansion gave way to an era of accountability, control and retrenchment.
These pressures gave rise to two separate streams of health reform.35 Market-oriented reforms were fuelled by macroeconomic and fiscal concerns.36 Initially, efforts were made to change the funding models and reduce public spending on health: to replace public funding with private sources (e.g., to replace tax-based funding with private health insurance), deregulate planning and budgeting, introduce or increase user fees and de-list or curtail entitlements.37 Other proposals included the introduction of vouchers, individual savings accounts and different forms of cash benefits, and the replacement of income-related contributions with flat-rate premiums. The common feature of these proposals is the move away from pooling risks of larger population groups toward increasing the risk of the individual. In other words, the proposals reflect an erosion of the insurance principle and a re-emergence of the residualist role of the state. In most countries, popular support for the solidarity-based health system and veto powers of other stakeholders proved a real barrier to change. When efforts to restructure the funding system met with failure, attention turned to the possibilities for improving the efficiency and organization of care. The United Kingdom introduced its “internal markets” within the NHS. Other countries followed this model of separation between the functions of purchasing and delivering health care.38
The second stream of health reform, with a quite different perspective, expanded on the very concept of health and challenged the borders of health policy. The early 1970s were a time of growing awareness that the health of a population depends on more than medical care alone. The Lalonde Report in Canada presented other factors (the “determinants of health”) such as personal lifestyle, genetic disposition, and social and economic conditions.39 The report gained in popularity and the WHO became a carrier of its ideas. In 1982, The WHO’s Health For All report embraced a wider vision of health: the absence of disability and illness. It also pressed governments to change their policies and suggested that the “medical paradigm” be replaced with the new “health paradigm.” Most WHO member states accepted this policy idea by signing the Alma-Ata declaration.40
In spite of these two reform movements, there was little actual change in the dominant medical model. Neither the market model nor the health paradigm have been able to replace the medical paradigm.41
Nevertheless, health-care systems did see some changes in the 1990s. In addition to fiscal and budgetary pressures, other factors played a role in reshaping health care and health insurance: changing consumer demand; the emergence of new players in the policy arena, with mounting outside interference in medical practice; growing influence of the corporate sector; and increased competition.42
The last decades of the 20th century brought major demographic and lifestyle changes within populations. In the mid-1970s demographers had to revise their projections as population growth rates dropped much more rapidly than expected. Two decades later they had to revise their forecasts for the levels of public expenditure on health care and related services. Populations were aging, and their financial situation and social behaviour were also changing.43
At the end of the century, life expectancy in OECD countries had risen to about 80 years. The number of elderly persons living alone grew as average family size dropped and the dominant model of several generations living together went out of fashion. The elderly generation had gained higher levels of education and financial security. They had become critical and informed consumers. The elderly are the fastest-growing group of Internet users, with a particular interest in information about health and health care. Government policies have strengthened this trend toward individual voice, choice and exit. For example, Germany, Israel and the Netherlands allow the sickness-fund insured to register with a fund of their choice. Several countries are experimenting with cash-benefit options instead of services in kind.
The economic problems of the 1970s and 1980s brought new actors to the health-care arena. Employers worried about growing health-care spending and high levels of absenteeism. They began to look at health care as an instrument for reducing disability and sick leave. The behaviourist welfare principle gained prominence, as illustrated by the rise of ”welfare to work” schemes and other efforts to rehabilitate and reintegrate ill and disabled workers. Health-care services were seen not as universal entitlements but as a means of achieving other policy goals.
One particular challenge to the dominant position of the medical profession came from the world of administration. In the 1980s, after noticing large unexplained variations in medical interventions, the American Health Care Finance Administration supported the development of medical practice guidelines and protocols as the basis for “evidence-based medicine.”44 The underlying assumption was that such guidelines would not only reduce practice variations among institutions and among physicians, but also improve the efficiency and efficacy of treatment, and thereby help to control costs. Non-medical actors with a financial interest in medical outcomes had begun to interfere with professional autonomy.
In the 1970s and 1980s several countries set up separate health ministries and separate agencies to administer health insurance, regulate the health-care professions, protect consumer interests and promote the health of the population. They also turned their attention to new areas of information technology and competition. This shift in mindset also served to cut the umbilical cord with the income-protection principle of the welfare state. Health care lost its status as a unique aspect of social security and became an “ordinary” sector of the economy, on an almost equal footing with housing or travel or any other service sector. If government intervention in the world of medicine (through the development of practice guidelines, for instance) was initially defended on the grounds of the need to reduce unnecessary treatment variations and to improve the quality of care, the next step was to introduce private-sector terms, instruments and techniques. Health care became business, with modern management jargon as its working language.45
The last two decades of the 20th century saw accelerated change in the organization of health care.46 Small-scale, stand-alone facilities are rapidly disappearing. Hospitals and other institutions have created regional networks of providers. They are engaging in horizontal and vertical integration of services, which often extend to extramural care. Mergers and takeovers have drastically reduced the number of independent health-care providers and insurance agencies. Other newcomers to the health-care market include private home-care providers, new intermediaries for circumventing waiting lists, private clinics, clinics for labour-related diseases and pharmaceutical disease-management firms.
The combined effects of the development of guidelines, protocols and benchmarks as instruments of performance measurement and the influence of modern management and organization have created an atmosphere of corporate enterprise. This process of “creeping corporatization” in health insurance and health care have brought the issue of competition back to the policy debate.47 In Europe this process has been accelerated by the policies of the European Union (EU). While European countries have agreed that social policies remain the primacy of national politics because of the overriding principle of “subsidiarity,” the EU has increasing influence. The main policy goals of the EU are peace and economic prosperity for all. The first goal has been largely achieved. The second is still in the making. The creation of one common market for persons, capital, goods and services that will benefit the citizens and economies of all member states requires the elimination of trade barriers and undue protectionist policies and practices. For more than three decades, health professionals have been able to travel freely within the EU, since member states acknowledge each others’ diplomas. Now, health-care providers can offer their services to citizens in other countries, and the European Court has ruled that health-insurance agencies cannot prohibit patients from seeking treatment abroad.48 This lowering of trade barriers is in striking contrast to the high and sometimes growing impediments imposed by provinces and professional selfregulating bodies within Canada.
Health expenditures in OECD countries vary greatly in levels, growth rates and ratios of public and private funding. Since the mid-1980s, under mounting fiscal and budgetary pressures, growth rates have been levelling off and there seems to be some convergence in spending levels. The data show that cost-control efforts have been successful (and that fears of rampant and uncontrollable cost escalation due to aging populations and technological advances are unfounded).
Both Canada and the United States combine elements of the liberal welfare state with collective health-care arrangements, an important difference being that Canada’s Medicare covers the entire population while US public schemes cover specific groups only. In most other OECD countries, health-care services are accessible, without undue financial barriers, to the entire population based on a mix of public financing (general taxation, social health insurance) and private financing (parallel or supplemental health insurance, co-payments, direct payment by patients).
The international experience reflects pressure for change across the OECD world. In the 1970s welfare policies came under mounting attack. The pressures, reform debates and options tested were similar, but there was no convergence of the basic funding models for health care. The failed health-reform efforts of the 1970s and 1980s had aimed to replace the funding structures. In the 1990s, however, health-care systems did undergo major changes. This time, the change was less a result of government policies and reform efforts than the outcome of pressure from consumers, employers and the corporate sector. There was a shift “from debate without change to change without debate.”49
In the 1980s and 1990s home care and pharmaceutical care rose on the policy agenda; in the OECD world, there was growing demand for both public and private home care. Remarkably, in the decades of retrenchment both Germany and Japan introduced universal long-term care insurance. While the actual expenditures on pharmaceutical care were relatively modest, their share rose rapidly, increasing the financial barriers for some patients.
Canada combines economic features of US markets with cultural elements of Western European policies. In terms of the Esping-Andersen typology discussed earlier, Canada’s social policies combine elements of the liberal welfare state (low levels of unemployment and disability benefits) with universal health-care entitlements. Carolyn Tuohy labels this dichotomy the “two worlds of welfare.”50 As to “dominant cultural orientation,” Canada features elements of both individualism and collectivism. Its economic and fiscal policies are similar to those of its neighbour, the United States, but its health-care system is more egalitarian in sharing the financial burden and providing universal and uniform access to services.
Canada has other features that set its social policy apart. It combines a relative weak position of federal governments with strong provincial powers and regional movements based on cultural, ethnic and linguistic identity.51 Moreover, it has many well-organized visible minorities. Over 30 percent of Canadians were born in another country. Social policies must reflect acceptance and accommodation of this diversity.52 Governments seek to achieve a delicate balance of gender and minority representation through extensive public consultations and community involvement in the shaping and implementation of social policies.
Western European countries have a centuries-long tradition of non-governmental actors participating in the funding and provision of social services. State intervention is a relatively recent phenomenon. It was only in the second half of the 20th century that the state became a central actor in welfare policies. This tradition has shaped the neo-corporatist model in which governments and stakeholder representatives share responsibility for shaping and implementing social policies. A “societal middlefield” of non-governmental organizations represents large segments of the population.
As a young country, Canada is not party to this tradition. Nevertheless, a large number of social services in Canada are provided by non-governmental agencies, with many efforts being made to at least consult and involve various groups in social policy. In fact, it could be argued that Canada is creating its own home-grown brand of neo-corporatism. Quebec clearly has kept some of the European traditions, though other provinces are less familiar with neo-corporatist policy-making.
Like other OECD countries, Canada features a mix of publicly and privately funded health care. In terms of the OECD categories, it combines the public contracting model with the reimbursement model for voluntary supplemental insurance. In the year 2000, total health expenditures were approximately CDN $95 billion, or $3,000 per person.53 Public sources, including taxation and mandatory health insurance, fund over 70 percent of all health expenditure. Patients pay about 30 percent either directly to providers or on additional health insurance. The Canada Health Act of 1984 sets the basic rules for Medicare, the universal social health insurance covering the costs of hospital and physician care at the point of delivery. The CHA frames five principles to which the provinces and territories must adhere in order to receive funding from the federal government: universality, accessibility, portability, comprehensiveness and public administration.
The provinces and territories act more or less as regional health insurance agents or third-party payers. Their function is similar to that of the sickness funds in Western Europe. They collect funds from the federal government and their own treasuries, contract with hospitals, physicians and other health-care providers, administer payments and monitor outcomes. They may also offer supplemental insurance. The federal government provides direct health-care services to status Indians and Inuit, the Royal Canadian Mounted Police, armed forces personnel, veterans, policemen and federal prisoners. In addition, there are provincial as well as work-related private health insurance schemes for services not covered under Medicare (e.g., pharmaceuticals) and direct payments by patients. Supplementary services are thus funded through a complex mix of public and private insurance and personal out-of-pocket payments.54
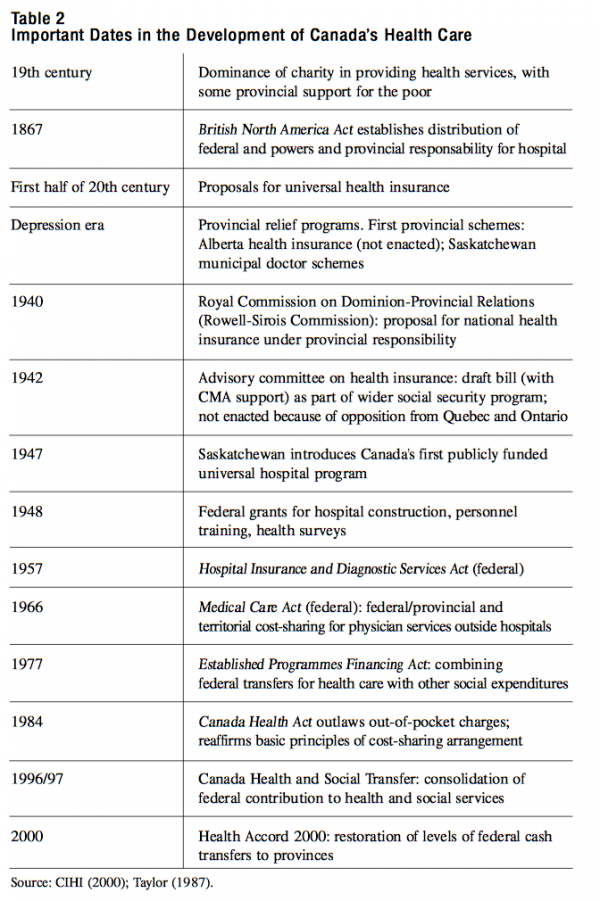
As with the health-care systems of other OECD countries, Canada’s Medicare is the outcome of decades of expansion (see Table 2). A typically Canadian feature is the gradual expansion of the scheme by category of services rather than by population group. Germany and France, in contrast, began their social health insurance with low-income workers, later extending it to other population groups. The US Medicare program benefits only the elderly, the disabled and patients with renal failure — though its founders expected it to be extended to other groups.55 Canada’s Medicare, in contrast, has its roots in a provincial insurance scheme for hospital care, the Saskatchewan Hospital Insurance Act of 1947.56 Other provinces followed suit, inspiring the federal government to act as well. Ten years after Saskatchewan’s move, Parliament passed the Hospital and Diagnostic Services Act. This legislation set the terms and conditions for the provinces’ participation in the federal cost-sharing arrangement. By 1961 all provinces were participating. It took almost another decade before the coverage extended to ambulatory care by physicians. The Medical Care Act was enacted in 1966, and all provinces had joined the scheme by 1971. Unlike the universal health insurance schemes of other OECD countries, Medicare does not cover pharmaceuticals or medical aids. The basic features of this federal-provincial cost-sharing model have remained in place, even though the share of federal funding has decreased over the years and federal, territorial and provincial ministers disagree over certain issues. After some years of acrimonious confrontation, the Social Union Framework Accord of 1999 (SUFA) and the Health Accord of 2000 showed a softening of tone. The federal government promised to (and later did) restore (much of) the federal transfers and to expand some programs.57
When compared to universal systems, Canada’s health-care system shows a high degree of paternalism. In general, governments assume that medical professionals and appointed or elected officials represent consumer interests. Canada lacks the Continental European tradition of a “societal middlefield” of organized stakeholders sharing responsibility for social policies. As a consequence, its social policy-making has little room for consumers as direct stakeholders even while the SUFA announced that the federal government would undertake action to broaden the scope for citizens involvement and consultation. There have been efforts to engage citizens and consumers in the debates, and in a few cases specific patient groups have developed effective lobbying power. But there has been little room for permanent and systemic representation of consumer groups in the shaping of health policies, and most consultation processes either involve a small selection of citizens on an ad hoc basis, or appointed experts only. For example, at the start of the National Forum on Health, one of the issues was how to make sure the forum represented not only all the provinces and territories but also sufficient numbers of women and minorities to be convincing as a national enterprise. The forum went to great length to set up country-wide consultations with experts and stakeholder groups.
Health Canada, when creating the governance structure for the 13 new Canadian Institutes for Health Research, appointed hundreds of members of boards, advisory bodies and working groups consisting of experts. The Canadian Policy Research Network includes three networks that more or less permanently bring together several dozen academics, policy-makers and other people each. Such agencies as the Health Transformation Fund, the Canadian Institute for Advanced Research, the Social Sciences and Humanities Research Council, the Population Health Initiative and the Canadian Institute for Health Information (CIHI) similarly involve hundreds of experts. There seem to be as many persons involved in the administration and research activities of these institutions as there are independent researchers.
In many provinces, the selection of board members for the new regional boards is hindered by the difficulty in finding representatives from all walks of life. In studying the backgrounds of health board members, a group of researchers from McMaster University found that the majority had direct interest as health-care providers.58 In fact, the most common form of consumer representation in Canada is “statistical representation,” meaning that careful selection of a representative from each population group deemed important to the particular policy issue is taken as fair representation of the group as a whole.
This high degree of paternalism is at odds with the position of the consumer in modern society. For several decades, associations of patients and elderly citizens have sought access to decision-making on social policies, with varying degrees of success. They have formed advocacy groups to represent their interests. In the 1990s modern technology opened new channels of communication with the Internet and telephone help lines. The CIHI has developed a database on Canadian health care that is accessible to the public. Its first annual report was downloaded over 100,000 times, a clear sign of widespread interest in information on health-care services. These examples illustrate the growing empowerment of consumers and consumer groups in society. However, the governance discussion has apparently not taken such changes into account. The recent proposals for home care focused on expansion of entitlements under Medicare. They pay little attention to the private provision of services. Few reports are based on consumer surveys of what services elderly or handicapped citizens really want and how they would like to pay for them. The voices of these people are channelled via experts on advisory committees and politicians who claim to represent their interests. This paternalistic attitude can be expected to cause growing tensions as more highly educated and affluent citizens claim a greater say in the funding and organization of home care and related services.
At present, home care and social services in Canada come under the jurisdiction of the provinces and territories.59 All provinces have developed a range of services in both acute and long-term care. Some have disease-specific programs, such as those for patients with diabetes or those for children. Others include these programs in their general home-care services. Most provinces provide the funding (with varying amounts of co-payments by users) but contract out the actual services to private or not-for-profit agencies. They vary widely in their provision of services and in their financial and organizational arrangements. Health Canada sees home care as a means to prevent, delay or substitute for intramural care.60 A study based on a national home care conference in 1998 reports on publicly funded home care only. The Canada Health Act considers home care part of “extended health-care services.” The federal government provides funding for such services but does not require the provinces to offer universal entitlements as part of health or social insurance.
Most provinces have regionalized models for the administration and contracting of public and private home care. Ontario has set up a province-wide system of Community Care Access Centres. Other provinces have established regional or local health authorities and boards. They provide a similar range of services, including assessment and coordination, home nursing and homemaking, personal support, “meals on wheels” and respite care. There is some variation in the mix of public and private provision of such functions. Some provinces offer the “single entry function” by public employees but contract out all other functions. Other provinces combine this function with a mix of public and private delivery of services. Eligibility criteria are similar as well, mostly based on assessment of need and availability of private resources such as relatives. Co-payment levels also vary according to means and income. Most provinces have limits on the total number of hours in a given period, ranging from 35–40 hours per week in Quebec to 60–80 hours per month in Ontario. All provinces are in the process of standardizing their assessment methods (in contrast to the situation in Japan, no effort is being made to standardize nationally). There is a general move toward integration of the assessment and coordination function.
Health Canada concludes that there are no generally agreed upon data on public home-care expenditures in all provinces and territories. Even fewer data are available on privately funded home care. Estimates of public funding vary from two to six percent of provincial health expenditure, with per capita amounts ranging from less than $35 in the Yukon and Prince Edward Island, to $50–60 in the Northwest Territories, Alberta and Quebec, to $64–80 in British Columbia, Saskatchewan and Nova Scotia, to $98–124 in Manitoba, New Brunswick and Ontario. There is some correlation between funding level and number of clients per 1,000 residents, but the available sources provide diverging data and it is not clear whether and to what extent demographic differences explain differences in expenditure levels.
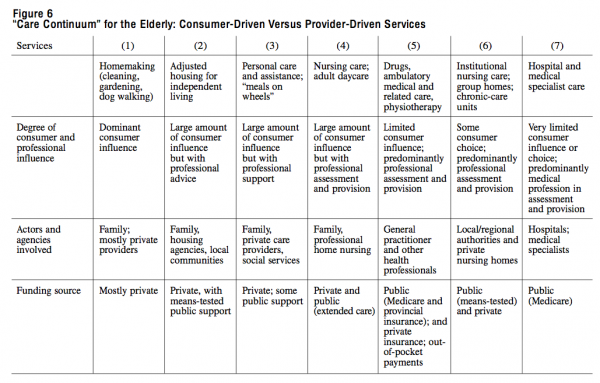
Home care is closely related to other social services like housing and transportation. For the frail elderly population, there are close connections between health care and adjusted housing, home cleaning, personal care and assistance, home nursing with links to nursing homes, ambulatory medical care, pharmaceuticals, hospital care and medical specialist care. In fact, from the perspective of the individual consumer there is a “continuum of care” spanning a much wider range of services (gardening, dog walking, filling in tax forms and other administrative chores) than those commonly provided by public agencies. These services can be ranked according to decreasing extent of direct consumer influence and increasing extent of decision-making power of (medical) professionals. Figure 6 shows that there is no clear line between public and private roles and responsibilities in the continuum of care. There are many agencies involved in the provision of health insurance, professional care and means-tested welfare support.
Some have argued that the entire range of medical and related social services should be brought under Medicare or another social insurance. However, there is reason to differentiate between services in which the consumer (or the consumer’s representative) has the leading voice, with means-tested government support if necessary, and services of a clearly medical character in which the consumer has little choice. Moreover, it would be naïve to assume that such a step would solve problems of coordination between services and agencies. Bringing services under one financial umbrella may place them within the same governance structure, but it will not automatically improve the management and coordination of patient streams and services. And from the client’s perspective, there will always be another range of services outside that structure. In Figure 6, the services in categories 1 to 3 are closely linked to local and regional welfare services, whereas those in categories 4 to 7 can be grouped under nursing and medical services. There are grounds for separating the first three categories from the others in terms of funding, contracting and governance. As these three are based on personal choice, with more options depending on individual purchasing power, the role of government can be seen as residualist, with means-tested income support as a supplement to the consumer’s income. The remaining categories are more dependent on professional assessment and decisions, with limited consumer choice. Here, the universal income-protection principle ranks first. That is not to say there is no relation between the two, as some consumers need services across the entire spectrum.
In the funding and provision of pharmaceutical care, existing arrangements differ greatly in terms of drugs covered, beneficiaries, eligibility rules and other conditions (see Appendix to the paper). Each province sets its own policy regarding administration and access for certain population groups. Each has to negotiate with the pharmaceutical industry on the formulary, market access of drugs and prices. The basic principles of the provincial schemes are much alike. Most provide partial or full coverage for drugs for senior citizens receiving Guaranteed Income Supplement (GIS), or to all seniors, or to all seniors that have no coverage by private insurance. In a few cases, in Alberta and the Northwest Territories spouses are included, too. Three provinces, Manitoba, Saskatchewan and British Columbia have extended the drugs benefits to all provincial residents. For those benefits, families in Manitoba face deductibles of two to three percent of net family income; residents in Saskatchewan pay 35 percent per prescription with a ceiling of $1700 per year. But the amounts of the deductibles and administrative fees per prescription differ and so are the categories of drugs and diseases covered.
In some cases, provinces have set an annual ceiling for the total of drugs expenditure of individuals. Such ceilings can take the form of an annual amount, e.g. $100 in Ontario. Other provinces have reduced the amounts for low income families, e.g. $100 instead of the full $850 semi-annually in Saskatchewan, and $600 instead of $800 in British Columbia. In addition, there is wide variety in coverage of drugs for other specific population groups, including social assistance and welfare recipients. In general, the latter groups face higher deductibles and co-payments than the elderly residents. Finally, all provinces and territories carry specific drug subsidy programs for certain categories of diseases. Again, those programs show much variation as to eligibility and range of drugs covered.
In brief, most provinces offer benefits to elderly residents, but the schemes vary as to eligibility, drugs covered and financial conditions. It is clear that the place of residence plays a greater role in a Canadian household’s pharmaceutical costs than in hospital of physician expenses.
The Canadian provinces and territories have developed a variety of homecare and drug schemes for their populations. This practical experience can as a starting point for discussion on the future of home care and pharmaceutical care. There are several questions to be addressed. Should the regional schemes be extended, or replaced with country-wide coverage under Medicare? What is the experience with national or regional arrangements in other countries? What stakeholders and agencies would be involved in implementing change? Is there a need to shift to universal entitlement (also bringing the danger of oversupply), or should change take the form of means-tested support for low-income groups? What are the borderlines between public and private functions, between funding and provider roles, and among private services, social services and home care?
Before these questions can be answered, four core elements need to be addressed: the institutional context of policy-making, the style of governance, the form of consumer involvement and the scale of operations.
Home-care services are very much linked with other social services, mostly of a local nature: adjusted housing for handicapped persons, special transportation, “meals on wheels” and home nursing. Each province has developed its own mix of public and private funding and contracting (though the basic principles and scope of services are similar across Canada). In the area of home care, the individual consumer has, or should have, some influence. Allowance for consumer voice and choice implies that individual wealth plays a role in the allocation of public funding. For this reason, means-tested welfare may be a more appropriate funding source than universal health insurance.
In contrast, a nationally administered scheme for pharmaceutical care may be more appropriate. One of the issues in managing separate provincial schemes is the scale of operations. In terms of population, Canadian provinces compare to small European countries. Within the EU, there is increasing collaboration both at the EU level and between state governments in the assessment of drugs for market access (in fact, national and EU procedures for market access have been fully harmonized). In the United Kingdom, the National Institute for Clinical Excellence seeks to aggregate efforts for determining the cost-effectiveness of treatment and drugs at the national level, as the government has found that regional health authorities lack the resources to conduct such studies, and also because it expects to greatly reduce overlap and duplication. Moreover, drugs policies must reconcile the goals of industrial growth and innovation with the social goal of health, which requires a broader and more balanced approach.61
Finally, as the experience in other OECD countries has shown, introducing universal schemes for public funding and provision of home care or pharmaceuticals does not require fundamental changes to the system. Nor would such steps bring the system to the brink of collapse. But that does not imply that Medicare is the only venue to do so. Given the very characteristics of pharmaceutical care and home care, neither are best served under the existing umbrella of Medicare.
The scale of operations and the link with other social services point to other options. One of the effects of federalism is the fragmentation in social policies and health care, or what Manga labels “Balkanization.”62 The provinces and territories have populations ranging from a few hundred thousand to several million. That compares to the “junior league” of small Western European jurisdictions: Monaco (24,000), Luxembourg (357,000), Norway (4 million), Denmark (5 million), Scotland (5 million) and Sweden (8.2 million). Such numbers are in sharp contrast to those of France, the United Kingdom, Germany, Spain and Italy, with more than 30 million inhabitants each.
Moreover, Canadian provinces are developing regionalized structures that operate on an even more modest scale. Such small-scale operations may be called for in the case of very localized social services such as adjusted housing for handicapped persons, local transportation, home-care services or “meals on wheels.” However, a much larger scale is clearly necessary for other goods and services, such as the running of health insurance schemes, the development of new technologies, or investments in medical education or hospital facilities. There are no clear or readily available criteria for determining proper scale, but common sense and crude actuarial understanding helps to assess orders of magnitudes. For example, in the case of health insurance, actuarial risks require that the population under one particular risk pool be large enough to act as a financial buffer against very expensive treatment or epidemics of common diseases like flu or measles. Experience shows that in order to be sustainable, health insurance schemes covering a wide range of medical services require a minimum of about 200,000 participants. This raises the question: How much financial risk can Canadian regions assume for the health costs of their populations?
Drugs policy is another area that requires a minimum scale of operation. The pharmaceutical industry has become very internationalized,63 with investments in research and development surpassing national borders. National governments and international agencies stress the need to collaborate on an international scale in tackling the complicated issue of how to combine industrial interests with health-care policies. Within the EU, there is growing interest in cross-border collaboration.
For other services, a pragmatic approach is called for, based on past experience and cautious assessment of what models may work best given institutional and other constraints. Here, it is useful to look at the experience across the border and at Canada’s own history and development. American states and Canadian provinces may provide a better basis of comparison with most European countries than, say, Canada with Denmark or the United States with Luxembourg.64 And, in fact, the current development of regional governance models in Canada provides a perfect laboratory of change. The very history of Canada shows that its national Medicare scheme grew out of provincial initiatives (see Table 2).
Like other industrialized nations, Canada has been under mounting pressure to address health care as part of social expenditures. Changing views on the role of government, economic stagnation, high levels of unemployment, and rapidly rising fiscal deficits in the 1970s and 1980s fuelled debates on the sustainability of the welfare state. Other topics of debate were the role of the state and the private sector in providing and safeguarding welfare and the position of individual citizens. Efforts to rein in federal spending included a freeze on federal transfers that eventually caused a shift in funding from the federal level to the provincial and territorial level. Several provinces tried to pass on this pressure to the regional level. In contrast to other OECD countries, however, Canada has had little discussion of alternatives to the basic funding model of Medicare.
Other reform proposals resembled those in other OECD countries: the imposition of prospective budgets on providers of care, the de-listing of certain services from public health insurance, and the introduction of private funding and other cost-control measures. The CIHI has concluded that the reform debates were, in fact, “overlapping generations of reform.”65 As in other OECD countries, many of these proposals met with resistance from the public and from health professionals. There is pressure to devolve authority and further decentralize health-care governance. In fact, decentralization and integration are the themes of many reform debates. At the same time, there is pressure to centralize and strengthen government control — for example, in the monitoring of outcomes and the publicizing of health-care services. But in Canada, as in other OECD countries, in spite of much discussion the basic contracting model — public funding and private provision of health care — has changed little.66
Roughly speaking, the reports represent diverging schools of thought on health reform. The Health Forum and the report of the Tommy Douglas Institute represent the “school of incrementalism,” advocating incremental improvements to the existing system. This approach includes increased levels of (public) health spending and improved efficiency of existing services in order to address demographic pressures and technological innovations. A second school of thought claims that the current health-care system is unsustainable and in need of fundamental restructuring: a shift from public to private funding and contracting, and a shift from collective arrangements to greater individual choice and individual risk. This school also attaches greater importance to competition and market-like mechanisms (although it does not suggest that the existing Medicare scheme be fully replaced). Interestingly, the two schools seem to adhere, for different reasons, to the “health paradigm” of the 1970s and 1980s.
The 1997 report of the Health Forum points to the urgent need for increased health-care funding.67 It begins by underlining the importance of the basic principles of the Canada Health Act, in particular the administration and collective funding of health care. It advocates increased emphasis on primary care and home care and an integrated child and family strategy. It points to the need for better accountability and for evidence-based medicine and recommends the creation of a Transition Fund to implement such policies. The report concludes that there is no need to change the funding model but suggests that improvements be made in consumer information and transparency as well as accountability. These recommendations led to the creation of the CIHI, an agency commissioned to collect and distribute systematic data on the health-care system.
The CIHI presented its first Annual Report in 2000. This report contains a wealth of detail on health-care services in all provinces. All CIHI information is directly accessible in printed and electronic form, and its first two annual reports have become best-sellers. Interestingly, the annual report itself does not contain recommendations for health-care reform. It points to the need for comprehensive information on health and health care, but in so doing it also changes the world of health care in Canada by providing its information directly to the public.
A recent Institute for Research on Public Policy report recommends improvements in the efficiency and quality of health-care services.68 It proposes the introduction of a patient charter (on the UK model) and increased accountability of health-care governance. It also advocates for more privatization and competition within the publicly funded system but stops short of proposing a shift from public to private funding. With the accountability recommendation, this report takes on one of the issues raised by the Health Forum.
The Clair Commission consulted extensively with experts, stakeholders and the general public in order to assess the need for reform in the funding and organization of health care in Quebec. Its report supports a shift from hospital-based to community-based care, through replacement of the solo practice model with groups of general practitioners in order to offer 24-hour access to primary care. The report calls for a renewed emphasis on health promotion and disease prevention.69
The Ontario Health Restructuring Commission came to similar conclusions but advocated a two-step approach: a restructuring of the province’s hospitals by closing the smallest facilities and regrouping specialist functions in larger centres, and a strengthening of primary care and integration of services. Interestingly, this commission was mandated to implement its recommended changes.
The Tommy Douglas Institute has taken a more modest and more pragmatic view, recommending a systematic cross-country comparison.70 Its report shies away from calling for a systematic overhaul of the health-care system, commenting that, in general, Canadians are satisfied with the services they are receiving. However, the report refers to a “crisis in public confidence” and concludes that while the basic structure of Medicare is solid, adjustments are needed.
The report of the Saskatchewan Commission on Medicare concludes that “all parties have underestimated the fragility of Medicare.”71 It recommends integration of the province’s health-care services and reorganization of hospital care, concentrating specialized medical services in three large hospitals and shifting some nursing and rehabilitation activities to community-care centres. The report advocates the creation of an autonomous Quality Council for monitoring health care and the promotion of evidence-based medicine. Further, it proposes the creation of “primary health services networks” and of “primary health teams” comprising providers (including family physicians), health district staff, emergency services and pharmacies. Other recommendations include a renewed focus on health promotion and quality of services, strengthening of governance, and increased attention to accountability, education, research and information technology, as well as “structured dialogue” on the future of Medicare. However, like some of the reports discussed above, the Fyke Report is short on detail.
In 2000, a Senate Commission headed by Senator Kirby began a two-year review of health care, including the experience of other countries. The fourth volume of the committee maps out a range of Issues and Options. Its final report is due for release in 2002.
In early 2001, a federal commission headed by the former premier of Saskatchewan, Roy Romanow, was formed “to examine the state of health care in Canada including the benefits and negatives of the current system.” Its findings are to be published in the fall of 2002. Even before this commission had formally begun its work, it suggested that Canada should not exclude the option of introducing or increasing user fees. Predictably, the floating of such a trial balloon caused an uproar. The Commission’s interim report appeared early 2002, and contains a wide range of issues and general questions that Romanow wants to discuss with “the Canadian people” in a number of public hearings during the year before finalizing the report.
Finally, the results of a number of recent studies support the idea of extending Medicare coverage to home care and drugs. One of the documents from a national conference on home care sponsored by Health Canada proposes a national program, with national guiding principles and a nationally defined “basket of goods.”72 Another supports the need for a national approach but rejects the system of federal funding.73
The above reform proposals contain some common elements. Most mention the underlying principles of Medicare framed in the Canada Health Act. At the same time, they pay little or no attention to the question of how such principles might translate into actual policies or governance models. The reports are rife with jargon and “persuasive definitions” — terms that express a certain ambition but do not provide an actual description.
At this point, it is time to pause and think about how to evaluate calls for change in the governance of Canada’s health care. Such an evaluation could be guided by seven principles:
These seven points entail a good degree of pragmatism. In addressing the pressure for change, they might be more helpful than generalized claims that the health-care system will go broke without wholesale reform. The points are especially relevant to some of the core issues of health reform: the parochial nature of the debate, the use of principles and general directions versus policy details, and the choice between incremental change and wholesale reform.
Debates about health-care reform are often parochial affairs. They tend to ignore actual experience on other jurisdictions at home or abroad, or to use it as ammunition rather than in a constructive fashion. Bias is clear in commentaries in both Canada and the United States about the health-care systems of their neighbour.75 In the Canadian health reform discussion, the United States is the most frequently cited example — usually in a negative way — followed by Britain and, seldom, continental European countries. Few of the reports cited in the preceding section ask how the current debate can profit from actual experience in Canada or elsewhere.
There is a big difference between learning about and learning from experience elsewhere.76 Making a brief visit to another country to discuss some interesting policy model or measure may be inspiring but will tell little about context. What is acceptable in one country may be entirely unacceptable in another. In June 2001, the Canadian Prime Minister paid a brief visit to Sweden to attend a meeting. In the wake of this trip, several newspapers ran articles on the success of the Swedish health-care system in controlling costs. The articles also remarked that Swedes pay user fees for hospital and physician services. Some journalists concluded that user fees had been successful in keeping costs down but did not pay much attention to other features of the Swedish health-care system. Sweden is a small country with a homogenous population and a long history of government control over social services. Regional and local governments bear primary responsibility for the funding and provision of health care to their populations. Most physicians and other health professionals are employees, receiving salaries instead of fees for service. We need to understand more than just one element of a system in order to draw conclusions about its success or failure.
Most of the reports cited in the preceding section reaffirm the importance of the basic principles of the Canada Health Act for the future of Canadian health care. They pay little attention, however, to the question of how these principles might translate into policies. They are strong in framing principles and directions — using much jargon in the process — but weak in explaining how their recommendations will affect providers, consumers and others in terms of decisionmaking power, contracting models and financial risks. Nor do they provide guidance as to the appropriate mix of private and public funding or the best governance model for public services.
An example of a commonly used but ill-defined term is “primary care-led reform.” Back in the 1970s the WHO advocated a shift away from hospitals and institutions toward primary care. Many countries have subscribed to the idea, but, three decades later, current reform proposals suggest little progress. Such experience underlines the need to be critical of rhetoric in the reform debate and to distinguish between rhetorical debate and actual outcomes. The term “primary care-led reform” conveys nothing about what steps might be necessary or how such reform will affect the stakeholders.
It is interesting to look at how the different reports prepared over the years in Canada perceive the existing health-care system. The Clair Commission for one concludes that the system needs a “new sense of purpose” and advocates “revolutions” in the funding and delivery of care. It suggests that the only way to address current problems and the “demographic time bomb” of an aging population is to strengthen the role of Quebec’s network of community health centres (CLSCs) in the provision of psychosocial and medical services. Many of the other reports contain similar terms, based on a similar analysis of the problems, and make similar recommendations.
The Health Forum report is framed in less alarmist terms. It finds the fears about collapse of Canada’s health-care system to be much exaggerated and concludes that, though adjustments are needed, the structure of existing funding and contracting models need not be changed. The Tommy Douglas Institute also deviates from the “emergency path,” noting in its report that alarmist media coverage has fuelled a “crisis in public confidence” and concluding that wholesale reform is unnecessary.77 It recommends a systematic cross-country comparison. In fact, current efforts to place funding and decision-making into regionalized governance models in health care and social services provide an interesting laboratory of change. Unfortunately, apart from the 1995 conference hosted by McMaster University and the Canadian Medical Association and recent Health Canada reports discussing options for home care,78 there have been virtually no efforts by policy-makers or academics to analyze Canada’s own experience in order to draw policy lessons.
As we have seen, OECD countries show great similarity in the basic principles of their health-care systems but major organizational, institutional and cultural differences. The policy issues and options are similar and the reform debate is framed in almost identical terms: the urgent need for restructuring. In spite of the “convergence in rhetoric,” however, there is little convergence in the basic models of funding.
Countries differ substantially in their historical development, institutions and culture. Country-specific characteristics affect not only the shaping and outcome of social policies but also the governance models. OECD countries show great variety in their mix of public and private funding, provision and governance of health care. Canada’s country-specific factors include federal-provincial relations, regional variations and increasingly diverse populations. The dominant cultural orientation includes elements of both rugged individualism and strong support for public governance. Federal and provincial taxation is the main funding source for health care, while the provision and management are mostly in private not-for-profit hands.
There is no way to define a “best model,” as the efficacy of any given model depends on the institutional context of policy-making. For example, the way governments interact with organized stakeholders varies from country to country. While their funding models diverge, in both France and the United Kingdom the central government plays the dominant role. Both Canada and Germany seek to involve a variety of stakeholders in the shaping and decentralized implementation of health policies, but in different ways. Germany’s neo-corporatist model is based on systematic involvement of stakeholder organizations in social policy. Lacking that tradition, Canada is attempting to develop alternative ways to channel and represent the interests of consumers and other stakeholders.
Most OECD countries subscribe to one set of principles regarding health policies: universal and equal access to good-quality services, consumer satisfaction and choice, provider autonomy and cost control (as the bulk of health care is publicly funded). They also see health promotion and consumer protection as major policy goals. In spite of broad support of such principles and goals, there is dispute about how to translate principles into policy, or how to improve existing governance models.
The governance model plays an important role in exploring the borderline between public and private health care (both in funding and in provision), as it links policy goals to outcomes through country-specific organizations and institutions. But while borrowing from corporate practice may help to improve management techniques, invoking principles of “good governance” will not turn public actors into corporate ones. Such terms blur analytical borders and can raise undue expectations. Similarly, terms like “societal entrepreneurship” and “stewardship” should be regarded as aspirational definitions rather than representative of change.
Appealing to the general principles of the Canada Health Act when discussing the expansion of health care does not provide guidance in actually shaping the “best model” for the funding and delivery of home and pharmaceutical care (within or outside Medicare). It is more productive to look at current practices and experience, both within Canada and abroad. It is clear that the changes required in health-care policy in Canada relate not so much to core principles but to different means of implementation.
The paternalism of the Canadian system, the lack of citizen-consumer interaction with day to day operations and accountability reduces flexibility, adaptability and effectiveness. Universal access is maintained in many OECD countries without some of the rigidities of the Canadian system. While most OECD countries have dominant public funding (out of general taxation, earmarked taxes or social health insurance) in order to protect incomes and safeguard universal access without undue financial barriers, they have a wide variety in the arrangements for contracting, ownership and management of health services. Such a mix of public coverage with private provision does not necessarily reduce universality or accessibility and can increase flexibility and effectiveness.
Proposals for drastic change tend to ignore the reality of current systems of funding and providing health care and current governance structures. Most elements of these systems and structures cannot be expected to change overnight. We should therefore assess what elements may change in the near future, and why. This conclusion leads to a modest and somewhat pragmatic view of the scope of health-care reform.
With special thanks to Brenda Gluska for substantial support in research and editing; to the students in my course, “The Politics of Canadian Health Policies,” Spring 2001; and to external reviewers and IRPP staff.
Altenstetter, C. and S.C. Haywood. Comparative Health Policy and the New Right: From Rhetoric to Reality. Hong Kong: Macmillan, 1991.
Anderson, Malcolm and Karen Parent. “Care in the Home: Public Responsibilities-Private Roles?” Paper prepared for the Dialogue on Health Reform, Kingston: Queen’s University, June 2000.
Arrow, Kenneth J. “Uncertainty and the Welfare Economics of Medical Care.” American Economic Review, no. 5 (1963): 941-973.
Baakman N, J. Van de Made and I. Mur-Veeman. “Controlling Dutch Health Care.” In Controlling Medical Professionals: The Comparative Politics of Health Governance, eds. G. Freddi and J.W. Björkman. London: Sage Publications, 1989.
Bacovsky, Rosemary A. Background Information. Prepared for the Conference on National Approaches to Pharmacare. Integra Consulting Ltd., December 2, 1997.
Banting, Keith. “The Welfare State as State Craft.” In European Social Policy: Between Fragmentation and Integration, eds. Stephan Leibfried and Paul Pierson. Washington, D.C.: Brookings Institution, 1995.
Bogdanor, Vernon. Can Government be run like a Business? London: Chartered Institute of Public Finance and Accountancy, 1994.
Borst-Eilers, Els and Kieke G.H. Okma. “Priorities in Health Care of Elderly People: Conflicting Images, Conflicts of Interests?” College Journal of the Royal College of Physicians of Edinburgh, no. 26 (1996): 553-558.
Brinkman, Eelco. Genoeg van de staat? Gastcollege in de cyclus Verantwoordelijkheid. Rijksuniversiteit Leiden, November 9, 1988.
Campbell, John and Naoki Ikegami. “Long-Term Care Insurance Comes to Japan.” Health Affairs, no. 3 (2000): 26-39.
Canadian Centre for Business in the Community. “Trends in Corporate Social Responsibility.” 1998. Available at https://www.conferenceboard.ca/ccbc/csr_topic/csr_trends.htm
Canadian Health Services Research Foundation. Issues in the Governance of Integrated Health Systems. Ottawa: Canadian Health Services Research Foundation, 1999.
Canadian Institute for Health Information. Health Care in Canada 2001: Annual Report. Ottawa: Canadian Institute for Health Information, 2001.
——. Health Care in Canada 2000: A First Annual Report. Ottawa: Canadian Institute for Health Information, 2000.
Canadian Medical Association and Queen’s University. How Many Roads? Report of the CMA/Queen’s Conference on Regionalization and Health Care in Canada. Kingston: School of Policy Studies, Queen’s University, 1995.
Commission d’étude sur les services de santé et les services sociaux (Clair Commission). Emerging Solutions. Available at https://www.cessss.gouv.qc.ca/pdf/en/01-109-01.pdf.
Commission on Medicare (Fyke Commission). Caring for Medicare: Sustaining a Quality System. Regina, Government of Saskatchewan, April 2001.
Committee on the Financial Aspects of Corporate Governance (Cadbury Commission). Report of the Committee on the Financial Aspects of Corporate Governance, 1992.
Decter, Michael B. Four Winds of Change. Toronto: Stoddart Publishing, 2000.
Dekker Committee. Bereidheid tot Verandering. Rapport van de Commissie Structuur en Financiering Gezondheidszorg.‘s-Gravenhage: Distributiecentrum Overheidspublicaties, 1987.
De Swaan, Abram. In Care of the State. Health Care, Education and Welfare in Europe and the USA in the Modern Era. Oxford: Polity Press, 1988.
Douglas, M. and A. Wildavsky. Risk and Culture. Berkeley Calif: University of California Press, 1982.
Ebenstein, William. Great Political Thinkers; Plato to the Present. 4th ed. New York: Holt Rinehart and Winston, 1969.
Esping-Andersen, G. The Three Worlds of Welfare Capitalism. Cambridge: Polity Press, 1990.
Freddi, G. “Problems of Organizational Rationality in Health Systems: Policy Controls and Policy Options.” Controlling Medical Professionals: The Comparative Politics of Health Governance, eds. G. Freddi and J.W. Björkman. London: Sage Publications, 1989.
Gress, Stefan and Kieke G.H. Okma. Managed Competition in Health Care — Dutch Present and German Future? Paper presented at the 9th Canadian Conference on Health Economics, Toronto, May 2001.
Hamilton, G.J.A. “Gezondheidszorg en mededingingsrecht.” In De rol van het mededingingsrecht in gereguleerde markten, eds. A.T. Ottow and A.F. Eeken. Den Haag: Boom Juridische uitgevers, 2001.
Hamilton, Geert Jan. “Ziektekostenverzekering in Europees Perspectief.” Medisch Contact. no. 46 (1995): 1469-1472.
Health Canada. Home Care Development. Provincial and Territorial Home Care Programs: A Synthesis for Canada. Ottawa: Health Canada, 1999.
Health Insurance Association of America. “Canadian Health Care: The Complications of Public Health Insurance.” Research Bulletin. Washington, D.C.: Health Insurance Association of America, 1990.
Heidenheimer, A.J., H. Heclo and C. Teich Adams. Comparative Public Policy. The Politics of Social Choice in America, European and Japan, 3rd ed. New York: St. Martin’s Press, 1990.
Heijmans, HF. Grenzen aan de Sociale Zekerheid. Geschrift nr 52. ‘s-Gravenhage: Teldersstichting, 1984.
Illich, Ivan. Medical Nemesis: The Expropriation of Health. Boston: Beacon Press, 1973.
IRPP Task Force on Health Policy. Recommendations to First Ministers. Montreal: Institute for Research on Public Policy, 2000.
Jacobzone, Stéphane. “Pharmaceutical Policies in OECD Countries: Reconciling Social and Industrial Goals.” Labour Market and Social Policy Occasional Papers no. 40. Paris: Organisation for Economic Cooperation and Development, 2000.
Jenson, Jane and Martin Papillon. “The Changing Boundaries of Citizenship. A Review and a Research Agenda.” Ottawa: Canadian Policy Research Networks, 2001.
Klein, R. “Learning From Others: Shall the Last be the First Markets?” In Four Country Conference on Health Care Reforms and Health Care Policies in the United States, Canada, Germany and The Netherlands, ed. Kieke G.H. Okma. Rijswijk: Ministerie van Volksgezondheid, Welzijn en Sport, 1995a.
——. The New Politics of the NHS, 3rd. ed. Harlow: Longman Group Limited, 1995b.
Koivusalo, M. and M. Rowson. “The World Trade Organization: Implications for Health Policy.” Medicine, Conflict and Survival, Vol. 12, no. 2 (April 2000): 175-191.
Lalonde, M. A New Perspective on the Health of Canadians. Ottawa: Government of Canada, 1974.
Lomas, Jonathan and Gerry Veenstra. If You Build It Who Will Come? Discussion paper. Hamilton: McMaster University, 1995.
Marmor, T.R. “Hype and Hyperbole: The Rhetoric and Realities of Managerial Reform in Health Care.” Journal of Health Services Research and Policy. Vol 3, no. 1 (January 1998): 62-64.
——. “The Politics of Medical Reform in Mature Welfare States: Facts, Fictions and Faction.” In Four Country Conference on Health Care Reforms and Health Care Policies in the United States, Canada, Germany and The Netherlands, ed. Kieke G.H. Okma. Rijswijk: Ministry of Health, Welfare and Sport, 1995.
Meurs Commission. Health Care Governance. Soesterberg: Health Care Governance Commission, 1999.
Ministry of Health. (Ministerie van WVC.) Verandering Verzekerd. Stapsgewijs op weg naar een nieuw stelsel van zorg. Kamerstukken II, 1987-1988, 19945, nrs 27 en 28.‘s-Gravenhage: SDU, 1988.
Moh, Vraag aan Bod. Letter by the Minister of Health to Parliament. The Hague: Ministry of Health, Welfare and Sport, 2001.
National Forum on Health. Canada Health Action: Building on the Legacy. Ottawa: National Forum on Health, 1997.
Noël, Alain. “Without Quebec: Collaborative Federalism with a Footnote?, Policy Matters, Vol. 1, no. 2 (March 2000).
Oakley, A. and S. Williams, eds. The Politics of the Welfare State. London: UCL Press, 1994.
Organisation for Economic Cooperation and Development. The Reform of Health Care: A Comparative Analysis of Seven OECD Countries. Health Reform Studies no. 5. Paris: Organisation for Economic Cooperation and Development, 1994.
——. The Reform of Health Care: A Comparative Analysis of Seven OECD Countries. Health Reform Studies no. 2. Paris: Organisation for Economic Cooperation and Development, 1992.
Okma, Kieke G.H. “Health Care and the Welfare State: Two Worlds of Welfare Drifting Apart?” Presented at the Conference on The Second Century of Social Security: Social Integration in the 21st Century, The Hague, June 14-15, 2001.
——. “Health Care Systems in Transition: An International Perspective.” (Book review essay) Journal of Health Politics, Policy and Law, Vol. 25, no. 6 (December 1999a): 1178-1183.
——. “Markets and Health Care: A Comparative Analysis.” (Book review essay) Journal of Health Politics, Policy and Law, Vol. 25, no. 6 (December 1999b): 1413-1419.
——. Studies on Dutch Health Politics, Policies and Law. Ph.D. Thesis, Utrecht: Utrecht University, 1997.
Okma, K.G.H. and A. De Roo. “From Polder Model to Modern Management in Dutch Health Care.” Presented at the 4 Country Conference 1998, The Future of the Hospital. New Haven, CT: Yale University, July 1998.
Peters Committee. Corporate Governance. The Hague: VNO, 1996.
Premier’s Advisory Council on Health (Mazankowski Commission). A Framework for Reform. Report of the Premier’s Advisory Council on Health. Edmonton: Mazankowski Commission. December 2001.
Raad voor de Zorg. Maatschappelijk Ondernemen. Zoetermeer: Raad voor de Zorg, 1997.
Rachlis, Michael, Robert G. Evans, Patrick Lewis and Morris L. Barer. Revitalizing Medicare: Shared Problem, Public Solutions. Vancouver: The Tommy Douglas Research Institute, 2001.
Ranade, W. ed. Markets and Health Care: A Comparative Analysis. London, New York: Longman, 1998.
Rodrik, Dani. “The Paradoxes of the Successful State.” European Economic Review, Vol. 41 (1997): 4112-4442,
Saltman, Richard B. and Odile Ferroussier-Davis. “The Concept of Stewardship in Health Policy.” Bulletin of the World Health Organization 78, no. 6 (2000): 732-739.
Skrabanek, P. The Death of Humane Medicine. London: The Social Affairs Unit, 1994.
Taylor, Malcolm G. Health Insurance and Canadian Public Policy: The Seven Decisions That Created the Canadian Health Insurance System and Their Outcomes. Kingston/Montreal: McGill-Queen’s University Press, 1987.
Thompson, Laurence G. Clear Goals, Solid Evidence, Integrated Systems, Realistic Roles. Health Care Papers, Health Services Utilization and Research Commission, 1999.
Timmins, Nick. The Five Giants. A Biography of the Welfare State. London: Fontana Press, 1995.
Tuohy, Carolyn J. “Social Policy. Two World of Welfare.” In Governing Canada: Institutions and Public Policy, ed. M.A. Atkinson. Toronto: Harcourt Brace Canada, 1993.
Wilson, Graham. Interest Groups. Oxford: Basil Blackwell, 1990.
World Health Organization/UNICEF. Primary Health Care, Report on the International Conference on Primary Health Care. Alma Ata, USSR. Geneva: WHO, 1978.
Zorgverzekeraars Nederland. Goed Verzekeraarschap (Code of conduct for health insurers). Zeist: Zorgverzekeraars Nederland, 1997.
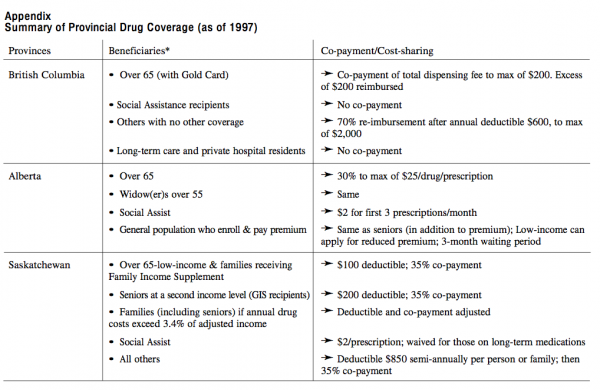
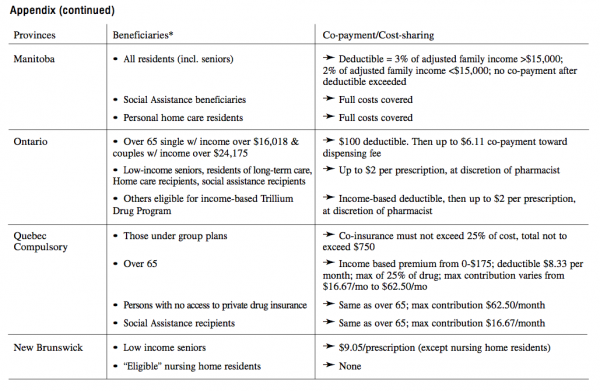
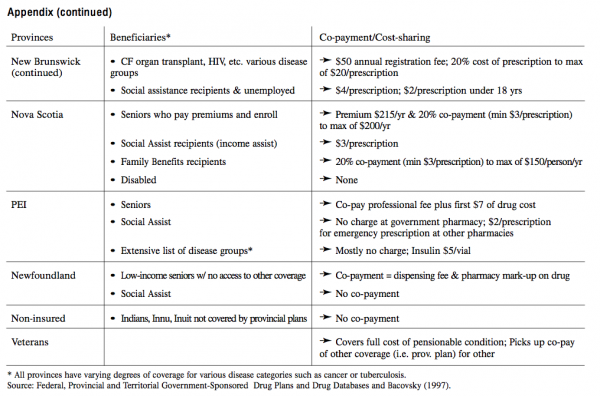
Kieke G.H. Okma is an Associate Professor at the School of Policy Studies at Queen’s University and is a civil servant with the Dutch Ministry of Health, her main employer for the last 10 years. Previously, she has worked with other Dutch departments including the Treasury, Foreign Affairs and Commerce. She spent five years in Washington, D.C. working for the World Bank, the IMF and the Embassy of the Netherlands. She has widely written and lectured on topics of social policies and international comparison.
For Immediate Distribution – Wednesday, May 22, 2002
Montreal – Experiences of Other OECD Countries Show There Is More than One Way to Achieve Universal Access to Services. Reforming the health-care system of Canada requires learning from the experiences of other countries while searching for reforms that are feasible and acceptable in Canada, according to “What Is the Best Public-Private Model for Canadian Health Care?,” a new paper released today by the Institute for Research on Public Policy (IRPP). The study’s author, Kieke G.H. Okma, proposes a framework for discussion of the future of Canada’s Medicare program and related health and social services.
The study examines the reforms to health-care governance implemented by some Organisation for Economic Co-operation and Development (OECD) member countries, the UK, France, Germany and the Netherlands among them, and analyzes proposals for Canadian health reform. The author also takes an original position by proposing to extend Medicare coverage to home care and pharmaceuticals.
Dr. Okma, Associate Professor at the School of Policy Studies at Queen’s University and a civil servant with the Dutch Ministry of Health, argues that there is more than one answer to questions on the public/private mix and administrative arrangements of health care, and that there is no universal “best model.” She underlines the fact that many OECD countries holding the same underlying values of fairness and universal access have systems that allow more choice to consumers and citizens, while using a less paternalistic approach than Canada. Nevertheless, it must be remembered that reforms possible in the political, economic and social environments of other countries may not be feasible in Canada. Reform is further complicated by unproductive rhetoric and the pointless invocation of principles – neither the Canada Health Act nor the governance debate offer guidance for prosaic questions when dealing with a system so resistant to change.
While simplistic pleas for wholesale substitutions of the current model and easy assumptions about the transferability of ideas or social programs should all be avoided, Canada can learn from policy experience abroad and from the experiences of its own provinces and territories. Still, there are not many windows of opportunity for the top-to-bottom restructuring of the current system so many are seeking. Opportunities for governments to implement major changes in social policy are rather restricted; what is thus required is a modest and pragmatic view of the scope of health-care reform.
“What Is the Best Public-Private Model for Canadian Health Care?” is the latest Policy Matters paper to be published by the IRPP. It is now available in Adobe (.pdf) format on the IRPP website at https://www.irpp.org – to access the document, simply click on the “What’s New” icon on the homepage.
– 30 –
For more information, or to schedule an interview with the author, please contact the IRPP. To receive IRPP media advisories and news releases via e-mail, please subscribe to the IRPP e-distribution service by visiting the newsroom on the IRPP website.
Founded in 1972, the IRPP is an independent, national, non-profit organization whose mission is to improve public policy in Canada by generating research, providing insight and sparking debate that will contribute to the public policy decision-making process and strengthen the quality of the public policy decisions made by Canadian governments, citizens, institutions and organizations.


