
Long-Term Care Financing: What’s Fair and Sustainable?
Frances Woolley

Uncertainty about the meaning of specific terms in the Canadian medical assistance in dying (MAiD) legislation puts Canadians at risk in a number of ways. Eligibility for MAiD may be determined too broadly or too narrowly, and there may be arbitrary inequality of access when the various MAiD assessors and providers interpret the law differently, say Jocelyn Downie and Jennifer A. Chandler.
Until the courts step in with definitive interpretations, they propose interpretations of six key phrases in the current law that urgently need clarification. The authors do not seek ways to expand or restrict access to MAiD but rather to determine the most defensible interpretations of the legislation, using the tools of statutory interpretation supported by the relevant clinical and other forms of expertise.
In conclusion, they invite all responsible authorities to adopt, endorse and/or disseminate the proposed interpretations in the report, in an effort to provide needed guidance to patients and health care practitioners and move the public discussion toward potential consensus on the meaning of the terms in the legislation.
In particular, they call on:
In February 2015, the Supreme Court of Canada (SCC) issued its decision in Carter v. Canada, declaring Canada’s Criminal Code prohibitions on voluntary euthanasia and assisted suicide invalid.1 The SCC declared that the prohibitions violated the Canadian Charter of Rights and Freedoms insofar as they prohibit physician-assisted death for
a competent adult person who (1) clearly consents to the termination of life; and (2) has a grievous and irremediable medical condition (including an illness, disease or disability that causes enduring suffering that is intolerable to the individual in the circumstances of his or her condition). “Irremediable”…does not require the patient to undertake treatments that are not acceptable to the individual.2
The SCC suspended its declaration of invalidity for 12 months to give the federal government time to pass legislation to regulate medical assistance in dying (MAiD) if it wanted to do so.3 After a change in government within that 12-month window (the Liberal Party having replaced the Conservative Party in power), the SCC granted a four-month extension.
In April 2016, the government introduced its MAiD legislation, Bill C-14.4 Reactions to the Bill were immediate and vociferous. Some felt that it was too permissive: for example, by not requiring judicial preauthorization of all cases (see, e.g., VPS-NPV 2017). Others felt that it was too restrictive: by requiring, for instance, that MAiD cannot be provided until “natural death has become reasonably foreseeable” (see, e.g., comments of Joseph Arvay and Jean-Pierre Ménard, Standing Senate Committee on Legal and Constitutional Affairs 2016b). Such disagreements were to be expected because there is disagreement within Canadian society about what eligibility criteria and procedural safeguards are most appropriate for MAiD.
It was also widely noted that the meaning of some of the Bill’s key terms and phrases was unclear. For example, questions were immediately raised about the meaning of “incurable illness, disease, or disability,”5 “advanced state of irreversible decline in capability,”6 “enduring physical or psychological suffering that is intolerable to them”7 and “natural death has become reasonably foreseeable.”8
Interpretation challenges are not uncommon with new legislation. However, the risks of leaving uncertainty and confusion unaddressed in this context are significant.9 Too narrow an interpretation could mean people who should have access may be denied MAiD; too broad an interpretation could mean some people may be given access who should not. Two persons in the same circumstances may be treated differently (one allowed access and one denied it) simply because their providers or their counsel interpret the legislation differently. Other consequences arising from the interpretive confusion are possible too. For example, in response to particular interpretations of the legislation that suggest no other option, some patients may forgo drugs needed for effective pain control and remain in a state of intolerable suffering in order to maintain the necessary level of decision-making capacity to reiterate their request at the time of MAiD administration. Finally, the uncertainty about the meaning of key terms and phrases may raise concerns about potential criminal liability, producing a chilling effect on medical and nurse practitioners’ willingness to provide MAiD.10
How can we avoid these consequences? Once a piece of legislation is in force, only the courts can definitively interpret it. Unfortunately, seeking clarification through litigation is prohibitively expensive and time-consuming. Few people denied access to MAiD because of issues of interpretation would be in a position to seek assistance from the courts. In the absence of definitive judicial guidance, there are nevertheless steps that can be taken to mitigate the problems mentioned above.
These challenges must be confronted by those who have the responsibility and authority to provide interpretive guidance to health care practitioners and patients: governments, directors of public prosecution and attorneys general, professional regulators, health authorities, professional liability protection providers, professional associations, and civil society groups. In the conclusion of this report, we provide recommendations for specific actions.
In short, there are instruments and avenues available to reduce uncertainty and confusion among patients and health care providers. Although 1,982 Canadians accessed MAiD in the legislation’s first year, between June 17, 2016, and June 30, 2017 (Canada 2017c), confusion remains and clarity is required. It is time for those who can help to clarify the meanings to do so.
To contribute to such an exercise of leadership, we developed a draft paper proposing interpretations for some of the most problematically uncertain phrases in Bill C-14. From this starting point, we refined the draft through discussions with some MAiD providers. We then posted it on the Social Sciences Research Network (Downie and Chandler 2017) and sought feedback through an open call (Twitter networks and e-mails to various people we know are interested in the topic) and direct contact with MAiD assessors and providers. In-person conversations with key experts from legal or regulatory entities led to further refinements.
We then hosted a Chatham House Rule11 meeting with 15 participants in Halifax in August 2017 to workshop the revised draft. The goal was confidence building, not consensus building. Our intention was to bring together people with relevant expertise from a variety of perspectives shaped by their roles or experiences within particular organizations. Everyone was asked to leave their institutional role at the door. Participants were invited to speak solely for themselves (and not for attribution), on the basis of their expertise. We spent a day and a half together discussing and debating the substance of the draft paper.
Following this meeting, we revised the draft paper again, recirculated it to the group for comments and incorporated further feedback. The result is the following set of interpretations of key phrases in the legislation. See box 1 for additional information about the process and this report.
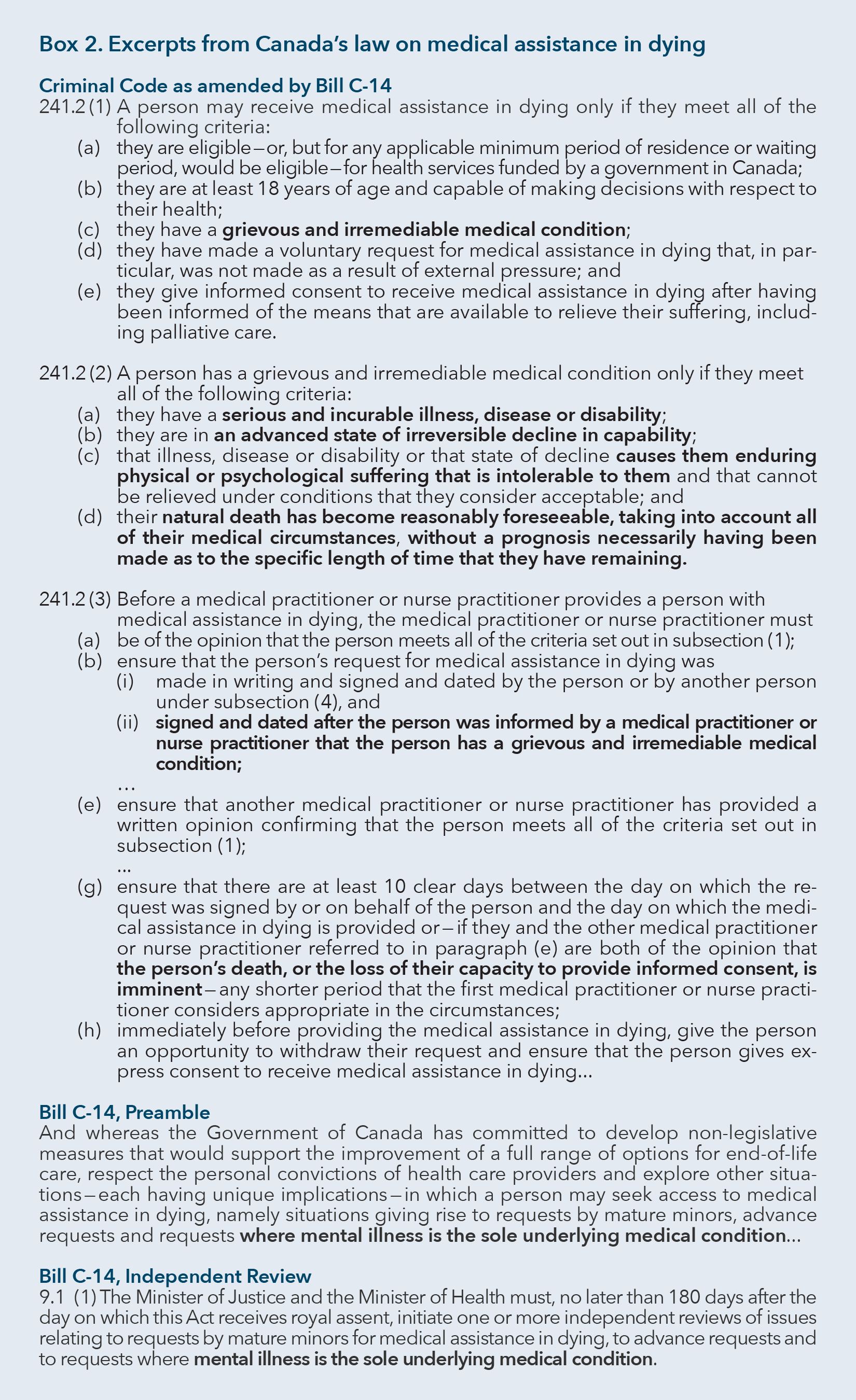
We have identified six phrases in the current law that urgently need clarification. They are presented in their statutory context in box 2.
In this section of the paper, we explain how these phrases are generating interpretive uncertainties. We then provide a proposed interpretation for each phrase, followed by a justification for each proposed interpretation.
The Canadian MAiD legislation requires that, in order to be eligible for MAiD, a person must have a “grievous and irremediable medical condition.” The legislation then lists four criteria for such a condition. One is that “their natural death has become reasonably foreseeable, taking into account all of their medical circumstances, without a prognosis necessarily having been made as to the specific length of time that they have remaining.”12 A key question, therefore, is when does natural death becomes reasonably foreseeable.

Although this is the fourth criterion listed in the legislation, we consider it first because it has generated the most interpretive difficulty.
On first impression, several possible meanings of “natural death has become reasonably foreseeable” emerge.13 First, the phrase could refer to some probability that a person will die a natural death as opposed to an unnatural death. Second, it could refer to timing: some probability concerning when a person will die a natural death; the most common interpretation of this kind is that natural death is likely within some specified length of time. Third, it could refer to cause: some probability concerning how the person will die a natural death (as a result of a particular set of physiological processes or conditions). Or it could refer to some combination of the above.
Uncertainty as to the interpretation of this phrase has consequences: medical or nurse practitioners who agree on a patient’s prognosis may nonetheless disagree as to whether the patient’s death is reasonably foreseeable because they disagree as to whether “reasonably foreseeable” refers to the that, the when or the how of the patient’s natural death.
Even among medical or nurse practitioners who think “reasonably foreseeable” refers only to timing and who interpret the law as requiring that natural death be expected within a certain length of time, interpretive complexities still remain. Does the concept of reasonable foreseeability require death to be anticipated within six months? Within 12 months? Within six years? A patient with a degenerative neurological condition (such as ALS) and a prognosis of four years could be said to meet the eligibility criteria on some of these interpretations, but not on others. The same could be said of a patient with cancer and a prognosis of nine months. There can be agreement on the prognosis and disagreement about whether the criterion is met, depending upon the specific length of time chosen as the boundary within which natural death must be probable.
Interpretation is no easier for those who think “reasonably foreseeable” refers only to the cause of death. “Natural death has become reasonably foreseeable” could refer to a requirement of a particular cause: for instance, that a person has a fatal condition that will most probably lead to natural death. Medical or nurse practitioners might disagree as to whether “reasonably foreseeable” requires a diagnosis with a fatal condition, and so reach different conclusions in situations where they all agree that a particular patient’s diagnosis is not that of a fatal condition. For example, an elderly patient may not have any single fatal condition but may have instead a constellation of chronic conditions and symptoms and a poor score on a frailty index (Rockwood et al. 2005). This patient’s natural death will not be reasonably foreseeable to some, but it will be to others.
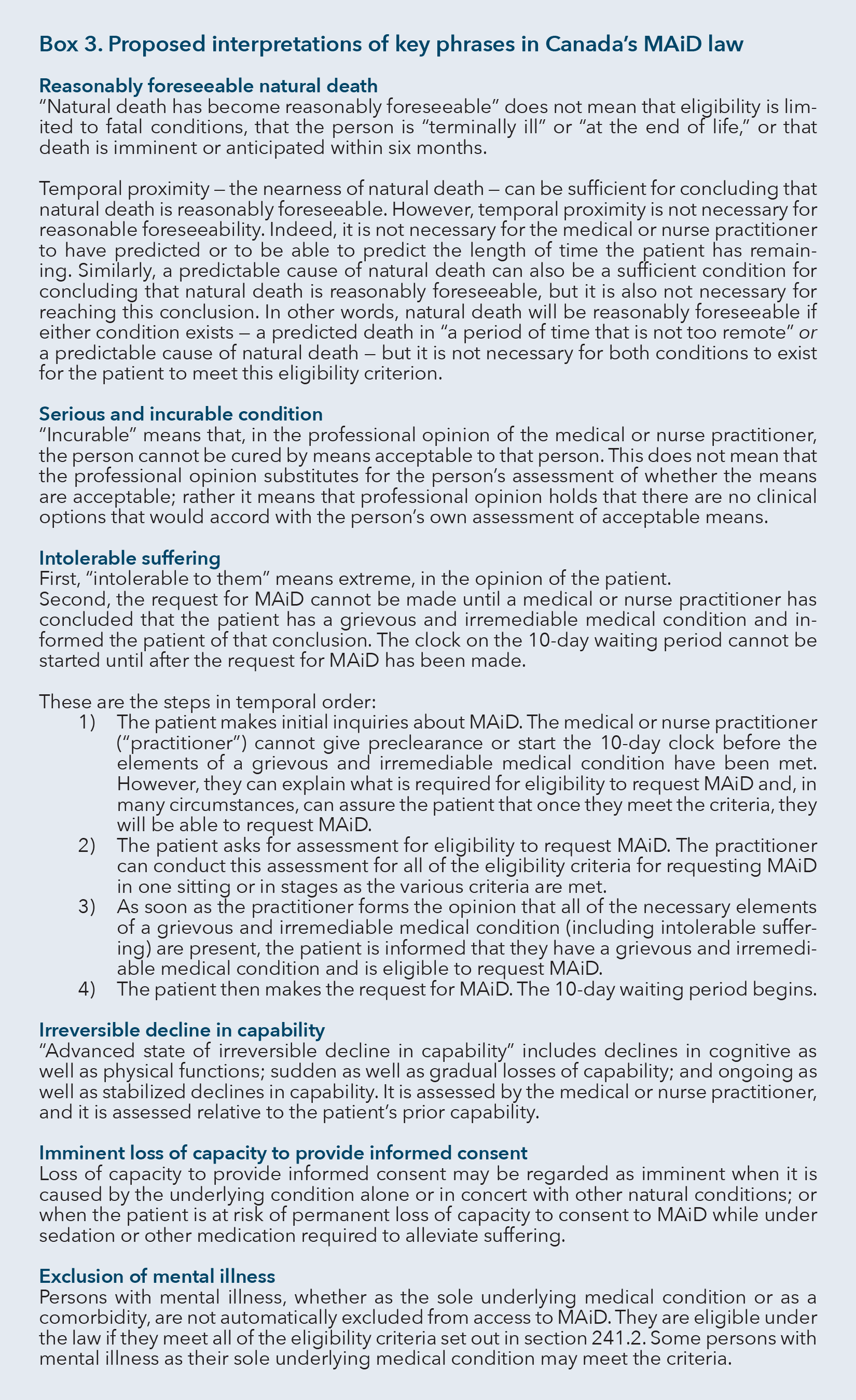
“Natural death has become reasonably foreseeable” does not mean that eligibility is limited to fatal conditions, that the person is “terminally ill” or “at the end of life,” or that death is imminent or anticipated within six months.
Temporal proximity — the nearness of natural death — can be sufficient for concluding that natural death is reasonably foreseeable. However, temporal proximity is not necessary for reasonable foreseeability. Indeed, it is not necessary for the medical or nurse practitioner to have predicted or to be able to predict the length of time the patient has remaining. Similarly, a predictable cause of natural death can also be a sufficient condition for concluding that natural death is reasonably foreseeable, but it is also not necessary for reaching this conclusion. In other words, natural death will be reasonably foreseeable if either condition exists — a predicted death in “a period of time that is not too remote” (Canada 2016b) or a predictable cause of natural death — but it is not necessary for both conditions to exist for the patient to meet this eligibility criterion.
There are several indications from the courts and the government of what “reasonably foreseeable” does not mean.
“Natural death has become reasonably foreseeable” cannot mean simply that someone will die a natural death, because more than 90 percent of people will do so (Martel 2015).
Justice Perell of the Ontario Superior Court of Justice recently issued a judgment interpreting this criterion in the case AB v. Canada (Attorney General).14 Although this is a single trial-level decision, the judgment makes it clear that the determination of the time window for anticipated death (the “when” interpretation) may be helpful but is not required to reach a determination that natural death “has become reasonably foreseeable”:
Natural death need not be imminent and…what is a reasonably foreseeable death is a person-specific medical question to be made without necessarily making, but not necessarily precluding, a prognosis of the remaining lifespan. […] In formulating an opinion, the physician need not opine about the specific length of time that the person requesting medical assistance in dying has remaining in his or her lifetime.15
Justice Perell also rejected one version of the argument that a particular cause is required (the “how” interpretation). He said it was not necessary that a patient have a terminal disease or condition
The language reveals that the natural death need not be connected to a particular terminal disease or condition and rather is connected to all of a particular person’s medical circumstances. […] The language does not require that people be dying from a terminal illness, disease or disability.16
The Crown has chosen not to appeal the AB decision. Of course, the Crown’s decision is not a concession that Justice Perell was correct or an endorsement of Justice Perell’s interpretation. In addition, AB is a decision from a trial judge in Ontario and so is not a binding legal authority. However, it is the only judicial interpretation available so far on the meaning of the “reasonably foreseeable” criterion.
Apart from the AB case, there are also plausible arguments based on statutory interpretation — relying on, for example, the legislative text and legislators’ intent — that support the conclusions drawn by Justice Perell about what “reasonably foreseeable” does not mean.
The law’s requirement that natural death be reasonably foreseeable includes the phrase “without a prognosis necessarily having been made as to the specific length of time that they have remaining.” This wording makes clear that temporal proximity is not a necessary condition.
Speeches made in the House and Senate about Bill C-14, as well as testimony before House and Senate committees and background and other explanatory materials produced by the government, can be reviewed to understand the policy intent. The criterion that “natural death has become reasonably foreseeable” should not, according to this evidence, be taken to mean that natural death must be
In line with these earlier statements is the government’s response to the civil claim made in Lamb v. Canada (Attorney General): “Eligibility for medical assistance in dying is not limited to those who are dying from a fatal or ‘terminal’ disease. No specific prognosis is necessary and death need not be imminent nor expected within a prescribed number of months.”23
Other statements in the same case suggest what the government believes “natural death has become reasonably foreseeable” does mean: “To have become ‘reasonably foreseeable,’ a natural death must be reasonably anticipated to occur by one of a range of predictable ways, and within a period of time that is not too remote” (emphasis added).24 Similarly, in the recent draft regulations to establish the federal monitoring system for MAiD, Health Canada proposes to require that, when a practitioner has assessed the patient for the “reasonably foreseeable” criterion for eligibility and is of the opinion that the patient meets that criterion, they must report “the reasons why the practitioner was of that opinion, including the practitioner’s estimate as to the amount of time by which medical assistance in dying, if provided, would shorten the patient’s life and the practitioner’s anticipation of the likely cause of natural death of the patient” (emphasis added; Canada 2017b).
Unfortunately, the government has provided no supporting arguments for this position. For the reasons set out below, we believe it is incorrect and that the “and” should be replaced with “or” in the government statements: “To have become ‘reasonably foreseeable,’ a natural death must be reasonably anticipated to occur by one of a range of predictable ways, and within a period of time that is not too remote” (emphasis added).25 Similarly, the regulations should be amended as follows:
the patient’s natural death had become reasonably foreseeable, taking into account all of their medical circumstances and, if the practitioner assessed this criterion and was of the opinion that the patient met it, the reasons why the practitioner was of that opinion, including the practitioner’s estimate as to the amount of time by which medical assistance in dying, if provided, would shorten the patient’s life (if a prognosis as to the amount of time that the patient has remaining was made) and the practitioner’s anticipation of the likely cause of natural death of the patient (if a likely cause was predicted).26
The legislative text is critical here. The “reasonably foreseeable” criterion says “without a prognosis necessarily having been made as to the specific length of time that they have remaining.” This could mean either that temporal proximity is not required, or that a prognosis of a specific length of time is not required but a prognosis of a nonspecific length of time is required. To characterize this required nonspecific length of time, some suggest the phrase used by the government: “a period of time that is not too remote.”
But how can a medical or nurse practitioner assess whether a patient’s death is likely within “a period of time that is not too remote” without knowing how remote is too remote? To identify a period of time that is “not too remote” and to assess whether this patient’s death is predictable within that period would require a prognosis of the specific length of time remaining — which would be inconsistent with the legislative text. To avoid this inconsistency, “a period of time that is not too remote” should be read as establishing the boundary of temporal proximity, which is a sufficient but not necessary condition for meeting the criterion of reasonable foreseeability.
Another potential interpretation of “reasonably foreseeable” is the presence of a predictable cause of death, such as a diagnosis of a fatal condition. The government made it clear that a diagnosis of a fatal condition was not a necessary condition for reasonable foreseeability. But there is no reason to believe that it isn’t a sufficient condition.
Putting this all together, the “reasonably foreseeable” criterion will be satisfied by either temporal proximity (“a period of time that is not too remote”) or a predictable cause of natural death, and neither is a necessary condition if the other is present.
Support for this conclusion can be found in government statements about the legislation. In particular, the language in a legislative backgrounder suggests that death should be expected “in a period of time that is not too remote,” but also allows for situations where there is a “long period of time before dying” (Canada 2016b, 10). The backgrounder also suggests that “a fatal disease” would make someone eligible, but the Minister of Justice and Attorney General, Jody Wilson-Raybould, clearly stated that “the bill does not require that people be dying from a fatal illness or disease or be ill” (House of Commons 2016a, 1010).
The Department of Justice published a glossary to Bill C-14, which includes this explanation:
Natural death has become “reasonably foreseeable” means that there is a real possibility of the patient’s death within a period of time that is not too remote. In other words, the patient would need to experience a change in the state of their medical condition so that it has become fairly clear that they are on an irreversible path toward death, even if there is no clear or specific prognosis. Each person’s circumstances are unique, and life expectancy depends on a number of factors, such as the nature of the illness, and the impacts of other medical conditions or health related factors such as age or frailty. Physicians and nurse practitioners have the necessary expertise to evaluate each person’s unique circumstances and can effectively judge when a person is on a trajectory toward death. While medical professionals do not need to be able to clearly predict exactly how or when a person will die, the person’s death would need to be foreseeable in the not too distant future. (Canada 2016a)
This analysis is from the legislative backgrounder:
The criterion of reasonable foreseeability of death is intended to require a temporal but flexible connection between the person’s overall medical circumstances and their anticipated death. As some medical conditions may cause individuals to irreversibly decline and suffer for a long period of time before dying, the proposed eligibility criteria would not impose any specific requirements in terms of prognosis or proximity to death…The medical condition that is causing the intolerable suffering would not need to be the cause of the reasonably foreseeable death. In other words, eligibility would not be limited to those who are dying from a fatal disease. Eligibility would be assessed on a case-by-case basis, with flexibility to reflect the uniqueness of each person’s circumstances, but with limits that require a natural death to be foreseeable in a period of time that is not too remote. It should be noted that people with a mental or physical disability would not be excluded from the regime, but would only be able to access medical assistance in dying if they met all of the eligibility criteria. (Canada 2016b, 10)
Arguably, the government’s various statements are somewhat confusing and appear at times to be internally inconsistent. However, we can reconcile them with the legislation and the one available court decision by concluding that either the when (“in a period of time that is not too remote”) or the how (a predictable cause of death) is enough to establish that reasonable foreseeability exists.
This conclusion also fits well with the kinds of circumstances that it seems the government intended to satisfy the criterion of reasonable foreseeability. The Minister of Health at the time, Jane Philpott, stated that individuals would meet the criterion from the moment of a diagnosis of ALS being made.27 The average life expectancy at diagnosis of ALS is two to five years; “half of all people affected with ALS live at least three or more years after diagnosis. Twenty percent live five years or more; up to ten percent will live more than ten years” (ALS Association, n.d.). Stephen Hawking, the world-famous physicist, was diagnosed with ALS at 21 and is still alive at 75. In addition, Minister Wilson-Raybould stated: “I am 100 per cent confident that Kay Carter [from Carter v. Canada] would be eligible under Bill C-14 to access medical assistance in dying” (Senate 2016a, 1420). Kay Carter had no diagnosis of a fatal condition. Spinal stenosis (her condition) itself does not significantly shorten life expectancy. She was, however, 89 years old. The proposed interpretation is consistent with these ministerial statements about who would be eligible.
The proposed interpretation also fits well with the conditions that, we can infer, the government intended to result in ineligibility under the reasonably foreseeable criterion. Comments by legislators suggest that the legislative intent was to exclude persons with a physical disability or mental illness who are otherwise in good health. Comments by Minister Wilson-Raybould indicate that the legislative intent was to exclude people like “a soldier with post-traumatic stress disorder, a young person who suffered a spinal cord injury in an accident, or a survivor whose mind is haunted by memories of sexual abuse” (House of Commons 2016c, 1014) and “persons who have recently become disabled in a car accident and have become quadriplegics” (House of Commons 2016d, 1102). What these individuals have in common is that it is not possible to identify in any way their trajectory toward a natural death: that is, the timing and cause of their natural death are both unpredictable when looking at the totality of their medical circumstances.
Additional examples may be helpful to illustrate the implications of the proposed interpretation in practice. These are conditions that meet the criterion of reasonable foreseeability, making patients eligible for MAiD if all other eligibility criteria are also met:
On the other hand, some persons who would not meet the reasonably foreseeable criterion and so are ineligible for MAiD would be a 25-year-old with quadriplegia following a car accident, a 45-year-old with chronic pain and a 50-year-old with multiple sclerosis — if they are otherwise healthy. In these cases, the period of time before death is too remote and the cause of death is not predictable.
It is important to note that, even if a person may satisfy the reasonably foreseeable natural death criterion, that person may not satisfy the other eligibility criteria (e.g., enduring and intolerable suffering, or advanced state of irreversible decline in capability).
Another criterion defining the “grievous and irremediable medical condition” required for MAiD eligibility is that the person have a “serious and incurable illness, disease or disability.”28
Does “incurable” mean incurable by any means? If so, as long as there is any chance of a cure from any available treatment, the patient would not be considered incurable.
Does it mean likely incurable by any means? Under this interpretation, if an available treatment offers any reasonable chance of cure, the patient would not be deemed incurable.
Or does it mean incurable by any means acceptable to the person? If so, if the only possible chance of cure comes from an available treatment that is unacceptable to the person (perhaps because the side effects of the treatment are, to the patient, worse than death), the patient would be deemed incurable.
In sum, is “incurable” defined relative to the patient’s perspective or to clinical judgment or to a combination?
Medical or nurse practitioners with different interpretations of “incurable” may agree on a clinical judgment (agreeing on all the biological facts, such as the chance of cure and the nature and severity of the side effects) yet disagree as to whether an illness, disease or disability is incurable. A patient with oral cancer who has already tried two different chemotherapeutic agents and is offered a third, with a 30 percent chance of cure, may decide that they cannot endure another round of chemotherapy. A Jehovah’s Witness may have a very good chance of recovery with chemotherapy for leukemia as long as they receive supportive blood transfusions; however, the patient refuses blood products for religious reasons (Knuti et al. 2002). On one interpretation (incurability as partially or wholly depending upon the patient’s perspective), these patients are “incurable” and thus eligible for MAiD; on another (incurability as exclusively a clinical judgment), they are “curable” and ineligible.
“Incurable” means that, in the professional opinion of the medical or nurse practitioner, the person cannot be cured by means acceptable to that person. This does not mean that the professional opinion substitutes for the person’s assessment of whether the means are acceptable; rather it means that professional opinion holds that there are no clinical options that would accord with the person’s own assessment of acceptable means.
The essential issue here is whether an illness, disease or disability is to be considered incurable when treatments are available that the medical or nurse practitioner thinks are potentially curative, but that are not acceptable to the patient. Another of the law’s eligibility criteria is “enduring physical or psychological suffering that is intolerable” to the patient; this criterion specifies that the suffering must be such that it “cannot be relieved under conditions that [the patient] consider[s] acceptable.”29 If the government had wished to include such a proviso in the “serious and incurable” criterion as well, some argue, it could have done so. They conclude that acceptability to the patient is not a condition of curability. We reject this argument for the following reasons.
First, the proposed interpretation is consistent with the well-established law on consent to medical treatment (in the area of criminal assault as well as the tort of battery). With very few exceptions (such as patients with certain communicable diseases), the law allows capable patients to refuse medical treatments for any reason whatsoever, regardless of the potentially fatal consequences of the refusal and regardless of whether others consider their refusal reasonable. As noted by the Senior Counsel of the Department of Justice:
I would conclude that the criminal law itself prohibits administering a medical substance to a person against their wishes. That is the crime of assault. The criminal law has to be interpreted consistently, as a whole. So it’s not possible to interpret “incurable” in Bill C-14, were it to pass, as though it would require a person, compel a person, to undertake a medical treatment that they otherwise don’t consent to. That is one section of the Criminal Code compelling what is criminally prohibited by virtue of another section of the Criminal Code. (Standing Senate Committee on Legal and Constitutional Affairs 2016c)
In other words, a person has the right to refuse any kind of treatment. A person can have an illness for which there is a potentially effective treatment, but if the person refuses to be treated, even to save their life, the illness will be, for all intents and purposes, incurable.
Second, in Carter v. Canada (Attorney General), the SCC used the language “grievous and irremediable condition” in establishing its criteria for MAiD and explicitly stated, “Irremediable…does not require the patient to undertake treatments that are not acceptable to the individual.”30 Parliament adopted the “grievous and irremediable” phrasing in its legislation. With no evidence that the legislature intended to deviate from the SCC’s approach to acceptability of treatment, it is reasonable to attach the same qualification to “incurable.”
Furthermore, this proposed interpretation of “incurable” has been explicitly adopted by the Minister of Health and the Senior Counsel for the Department of Justice. When appearing before the Senate, both stated that “incurable” should be interpreted as including the limitation “by any means acceptable to the patient” (Senate 2016a, 1650; Standing Senate Committee on Legal and Constitutional Affairs 2016c).
Finally, the question of the meaning of “incurable” was explicitly raised by legislators who were concerned that it was either an objective (clinician-only) or mixed objective-subjective (clinician and patient) standard rather than a purely subjective (patient-only) standard (Senate 2016a, 1650; Standing Senate Committee on Legal and Constitutional Affairs 2016c). Their questions were answered by the government’s representatives as indicated above. It therefore seems reasonable to assume that the fact that no amendment was offered with respect to the standard31 indicates that the broader legislative understanding and intent was for the standard to include the patient’s perspective on acceptability.
Before concluding this justification of our proposed interpretation, three additional points must be made. First, our proposed interpretation contemplates that both the person seeking MAiD and the medical or nurse practitioners assessing eligibility for MAiD have a role to play with respect to whether this eligibility criterion is met. The medical or nurse practitioner determines whether the patient has a condition and whether it can be cured by means acceptable to the person; the person requesting MAiD determines whether any potential treatments are acceptable.
Second, the established norms of informed consent apply in the context of MAiD; the provider must ensure that the patient has been informed of the treatment options and is capable of understanding and appreciating the consequences of refusing potentially effective treatment.
Third, good clinical practice also requires that the provider investigate a patient’s reasons for refusal of treatment to verify whether any of the concerns leading to rejection of a possible treatment may be mitigated (for example, whether a misunderstanding about the side effects of the treatment can be cleared up).
Among the legislation’s criteria for “grievous and irremediable medical condition,” which is required for accessing MAiD, is that the person must have an “illness, disease or disability or…state of decline [that] causes them enduring physical or psychological suffering that is intolerable to them and that cannot be relieved under conditions that they consider acceptable.”32
Two categories of uncertainty arise from the criterion of intolerable suffering.33
First, the meaning of “intolerable to them” can be understood in more than one way. Specifically, does it mean suffering that literally cannot be tolerated, or does it mean an intensity of suffering that is at the far end of a spectrum running from mild to extreme?
Second, questions have been raised about the timing of the assessment of the intolerable suffering criterion relative to the assessment of the other elements of eligibility to make a request for MAiD and the actual making of a request for MAiD. The legislation provides the following sequence of steps:
The legislation also requires that, in order to receive MAiD, two independent medical or nurse practitioners must be of the opinion that the patient requesting MAiD meets all of the eligibility criteria (sections 241.2(1) and (2) as set out in box 2). Thus, in order to be eligible to make a request for MAiD, the patient must have been found by one medical or nurse practitioner to have a “grievous and irremediable medical condition.” In order to be eligible to receive MAiD, the patient must have been found by two medical or nurse practitioners (independent from each other) to meet all of the eligibility criteria (not just the criterion of “grievous and irremediable medical condition”).34 For the rest of 3.3.1, we are concerned only with the matter of eligibility to make a request for MAiD.
An issue with respect to timing arises because of the requirement that the request cannot be made until a person has been found to have a “grievous and irremediable medical condition.”35 Since a required element for that finding is the existence of intolerable suffering, some people are concerned about what the required timing implies: that the patient must wait until the pain is intolerable before the request can be made and then wait 10 days between the request and the provision of MAiD (unless they meet the exception for imminent loss of capacity or death discussed below in section 3.5). This timing increases the risk of unexpected loss of capacity to consent, which would mean ineligibility for MAiD. Further, it means that patients have to endure 10 additional days of suffering that is, by definition, intolerable, because the waiting period cannot begin until that level of suffering has been reached.
Some patients would like to know — before their condition becomes grievous and irremediable (especially with the intolerable suffering component) — that they will have access to MAiD. Knowing this, they say, would bring them comfort through the months and weeks leading up to their death. Some patients would like to make the request for MAiD before intolerable suffering begins, so that they would not have to endure 10 days of it.
In response to these concerns, some have interpreted the legislation to allow the request to be made before all of the criteria of “grievous and irremediable medical condition” have been met. Others have said that the legislation allows the process of determining whether the patient’s medical condition is grievous and irremediable to begin before all of the elements of such a condition are being claimed (e.g., before the patient has concluded that she is in a state of intolerable suffering), but that the request for MAiD cannot be made until a medical or nurse practitioner has informed the patient she has a grievous and irremediable medical condition (as defined in the legislation). Still others have suggested that the process of determining whether the patient’s medical condition is grievous and irremediable cannot begin until all of the elements of such a condition are being claimed (including that the patient’s suffering has become intolerable). Still others have suggested that the request for MAiD cannot be made until the process of determining whether a patient meets all of the eligibility criteria to be able to receive MAiD has been completed by the two independent medical or nurse practitioners.
Given the diverse and, we think in some cases, incorrect interpretations that are sometimes being relied upon, the legal requirements about timing need clarification.
First, “intolerable to them” means extreme, in the opinion of the patient.
Second, the request for MAiD cannot be made until a medical or nurse practitioner has concluded that the patient has a grievous and irremediable medical condition and informed the patient of that conclusion. The clock on the 10-day waiting period cannot be started until after the request for MAiD has been made.
These are the steps in temporal order:
The word “intolerable” has two well-established meanings. The first relates to impossibility: “that cannot be tolerated, borne, or put up with; unendurable, unbearable, insupportable, insufferable.”36 The second way in which the word is used is “as a strong intensive: excessive, extreme,”37 “excessive”38 or “extremely irritating or annoying.”39 The latter meaning suggests that something that is intolerable is positioned on a spectrum toward the extreme end, rather than that it is literally impossible to bear.
We can reasonably adopt the second meaning, for two reasons. First, the law specifies that a person may make a signed request for MAiD only after suffering has become “intolerable to them” and then must wait another 10 days before confirming their request and receiving MAiD. This suggests that the law regards intolerable suffering as something that it is possible to bear. If the meaning intended by the law was suffering that is literally impossible to bear, there would be no patients for MAiD as they would necessarily request deep and continuous sedation and in this condition they would become ineligible for MAiD. Or, as we argue below, the 10-day waiting period would be waived because medically suitable deep and continuous sedation would lead to loss of capacity before the waiting period ends. To read “intolerable” as literally impossible to bear is therefore inconsistent with the procedure contemplated by the law, namely that at least some patients will undergo a 10-day waiting period before receiving MAiD. Second, it is reasonable to assume that the legislature intended the more humane result of compelling patients to endure 10 days of suffering that is “extreme” in the patient’s view but not literally “unbearable.”
The implication of the different definitions is significant. For example, if “intolerable” means something that cannot be tolerated, then it is not logically coherent for a patient to say, “This pain is intolerable to me, but I will put up with it for six weeks until my first grandchild is born,” or a similar landmark event. If it means extreme, then it is logically coherent for a patient to say that.
It is also clear from the law that the degree of suffering and the patient’s response to it are to be determined subjectively, rather than by applying objective or third-party notions of what is or is not extreme. The law uses the phrase “intolerable to them” (emphasis added), referring to the patient. So it is the patient’s own perception of their mental or physical suffering as extreme that matters.
In regard to the timing of the MAiD process, the legislation is clear and explicit that: (1) the request cannot be made until after the diagnosis of a grievous and irremediable medical condition has been given; and (2) the clock on the 10-day waiting period cannot start until after the request has been made.
It is reasonable to infer from the text that the clock on the 10-day waiting period can start before the assessments of eligibility to receive MAiD have been completed, indeed even before all of the eligibility criteria to receive MAiD have been met.40 Also, if a medical or nurse practitioner who is asked to assess the patient for eligibility to receive MAiD is of the opinion that the patient does not meet the eligibility criteria to receive MAiD, the patient can ask for another eligibility assessment and bringing in additional medical or nurse practitioners in such circumstances does not require the waiting period clock to be restarted.
Nothing in the legislation prevents medical or nurse practitioners from having robust preliminary conversations with patients about MAiD and reassuring them through clear explanations of how the eligibility criteria to request MAiD relate to their prognosis. There is also nothing in the legislation to prevent assessments of eligibility criteria to request MAiD to be conducted in stages. One advantage of assessing the various elements of eligibility over time as they become manifest is that a patient may initiate and go through part of the assessment process before their suffering becomes intolerable. This means that, once the patient is in a state of intolerable suffering, the final confirmation of eligibility to request MAiD may be made more expeditiously, since the other criteria will already have been investigated. In addition, the patient may be comforted by the knowledge that a significant part of the process of assessing eligibility to request MAiD has been completed. One disadvantage is that the stepwise determination of eligibility will put additional burdens on the practitioner assessing eligibility to request MAiD, as it is possible that multiple interactions with the patient will be required. In addition, it also relies upon the availability of the practitioner to make the later assessment of intolerable suffering.
An additional criterion for meeting the requirement that a person accessing MAiD has a “grievous and irremediable medical condition,” and the final one we consider here, is that the person be in “an advanced state of irreversible decline in capability.”41
There are multiple areas of uncertainty regarding this provision.
First, is “capability” limited to physical function, or does it also include cognitive function?
Second, do the terms “advanced state” and “decline” mean that the loss of capability must be a gradual, protracted process? If so, a patient who has a sudden, precipitous loss of capability would be ineligible for MAiD. If meeting this criterion requires only a substantial loss of capability, no matter the speed of the decline, a patient who experiences a precipitous loss would still be eligible.
Third, can the decline in capability have stabilized, or must it be continuing?
Fourth, is the decline in capability assessed according to a subjective or an objective standard — that is, by the patient or by the practitioner?
Fifth, is the decline in capability assessed relative to the patient’s prior capability or relative to the general population’s capability?
Some examples may illustrate the impacts of these uncertainties. One patient has had a stroke that left him with severe prosopagnosia, which means that he can no longer recognize faces, including his own. Another patient has had a stroke also and is now unable to speak the language she had spoken for the past 30 years, but she can speak the language she spoke for the first 10 years of her life.42 For both of these patients, their physical function has not been compromised, but their cognitive function has been compromised while they have retained medical decision-making capacity.
A third patient had a severe brain-stem stroke two years ago. His cognitive function is not compromised and he retains the ability to communicate; however, he has permanent widespread paralysis. His decline was sudden rather than gradual, and it was substantial. Three years pass and, while his decline was severe, it has stabilized, so now he is in a state of having experienced a severe decline but not declining further.
Which of these patients has reached an advanced state of irreversible decline in capability? Is this a judgment to be made by the medical or nurse practitioner or by the patient? And what is the standard for assessing decline: the patient’s prior capability, or that of the average person, or some other generalized norm?
“Advanced state of irreversible decline in capability” includes declines in cognitive as well as physical functions; sudden as well as gradual losses of capability; and ongoing as well as stabilized declines in capability. It is assessed by the medical or nurse practitioner, and it is assessed relative to the patient’s prior capability.
First, it is justifiable to regard the meaning of “capability” in this context to refer to the full range of human abilities, including physical and cognitive functions. In a standard dictionary, “capable” is defined as “having attributes (such as physical or mental power) required for performance or accomplishment.”43
The term “capability” is used in a broad range of Canadian statutes and regulations to refer to the abilities of both human beings and nonhuman entities and to refer to both physical and mental (including cognitive) capabilities of human beings. Various pieces of legislation use the term “capability” in a context plainly intended to refer solely to mental (including cognitive) capabilities.44 So it does not appear that there is a settled legal meaning that would restrict “capability” to physical abilities. Elsewhere in the Criminal Code, the phrase “physical capabilities” is used, suggesting that when legislators intend to limit the meaning of capability to physical capability alone, the text of the law will say so explicitly.45
Bill C-14 could have said, but did not, “an advanced state of irreversible decline in physical capability.” Therefore, it is reasonable to interpret this criterion as including both physical and cognitive decline.
Some raise the question of whether persons in an advanced state of decline in cognitive function would meet the eligibility requirement that an individual must retain decision-making capacity. If they lack this capacity, it is argued, the only meaningful reading of “capability” is that it refers to loss of physical function.
However, this view reflects a misunderstanding of the nature of at least some types of cognitive dysfunction. For example, a wide range of visual perceptual disorders are common in patients who have had strokes. These include:
A patient with such a disorder is in an advanced state of decline in cognitive function but could still have decision-making capacity for MAiD.
This being said, many other types of decline in cognitive function could negatively affect decision-making capacity. A person in this state would be ineligible for MAiD as a result of inability to give valid informed consent, but not because their advanced state of irreversible decline is of cognitive, not physical, capability.
Second, the pace of “decline” can be protracted or precipitous. If the government had wanted to limit eligibility to those experiencing a drawn-out decline, it should have explicitly said “advanced state of gradual irreversible decline in capability.”
Those who interpret “advanced state” and “decline” as requiring a gradual process of loss of capability may be doing so out of an underlying concern that patients may not have the decision-making capacity to choose MAiD in the immediate aftermath of a sudden and serious injury. This will be true of some patients but not all. More importantly, though, that concern should be addressed directly in every case through the application of the requirement for voluntary and informed consent (which requires decision-making capacity) instead of introducing both confusion and duplication by addressing a capacity concern through restrictive interpretations of the terms “advanced state” and “decline.” Indeed, there are normal rules about decision-making capacity that apply in the context of other life-ending decisions after sudden serious injury (e.g., rules for withdrawal of life support following a traumatic injury causing quadriplegia). These already established approaches would also be applied in the context of MAiD.
Third, a “decline” can be a stabilized state or an ongoing process. It can be a position on a slope lower than a previous position or an ongoing descent down a slope. If the government had wanted to limit this criterion to a continuing process, it should have explicitly done so by saying “advanced state of ongoing irreversible decline in capability.”
Fourth, whether there has been a decline in capability is a clinical question that should be measured objectively. It is therefore best answered by the medical or nurse practitioner.
Finally, it makes no sense to assess the decline in capability relative to an average person’s capability or some other generalized norm. What would the standard be? Would it be best-case capability or median or mean? Would it be relative to the entire world? The country? The region? Would it be relative to groups the individual belongs to (e.g., gender, race, disability)? What if the person, before the onset of their incurable condition, was below average on a variety of capabilities? Again, if the government had wanted this criterion to be judged against capabilities held by individuals other than the patient, it should have explicitly given direction as to what standard, other than the patient, was to be used.
Before concluding this subsection, we emphasize again that all four elements of the definition of “grievous and irremediable condition” must be met for a person to be eligible for MAiD. Therefore, patients with severe prosopagnosia following a stroke, for example, might be assessed to be in an advanced state of irreversible decline in capability because of their severe loss of cognitive function. But, without other medical circumstances, they would not qualify for MAiD.
The MAiD legislation establishes that the medical or nurse practitioner who actually provides MAiD must “ensure that there are at least 10 clear days between the day on which the request was signed by or on behalf of the person and the day on which the medical assistance in dying is provided.”46 The person must reiterate their request for MAiD immediately before it is provided, and must therefore have decision-making capacity at that time.47 However, the legislation provides an exception for this 10-day waiting period: if the two required independent assessors “are both of the opinion that the person’s death, or the loss of their capacity to provide informed consent, is imminent — [then] any shorter period that the first medical practitioner or nurse practitioner considers appropriate in the circumstances [is permitted.]”48
Although the 10-day waiting period was probably meant to ensure the stability of the decision to seek MAiD (and to prevent action on impulsive decisions), because of the way the legislation was drafted, it has the effect of making patients who wish to access MAiD confront 10 additional days of intolerable suffering.49 It is likely that this was an unintended consequence of an amendment made during the chaotic process of passing the legislation.50
The version of the legislation first introduced required that, before a request could be signed, the person must have been informed that their natural death had become reasonably foreseeable, taking into account all of their medical circumstances. A 15-day waiting period would then commence. MAiD could not be provided until the suffering had become intolerable. But the request could be made and the waiting period started before the suffering had become intolerable.
However, the version of the legislation that was ultimately passed required that, before a request can be signed, the person must have been informed that they have a grievous and irremediable medical condition; given the definition of that phrase in the legislation, that means that they would already be experiencing enduring and intolerable suffering. A 10-day waiting period then commences. The person therefore, by operation of the legislation, faces at least 10 days of intolerable suffering.
Because of the amendment — passed with no discussion or apparent appreciation of its effect — some patients are being presented with a terrible choice: accept effective, medically appropriate symptom control in order to reduce their suffering but risk losing capacity to give the required express consent immediately before the provision of MAiD and, if that happens, forever lose the opportunity for MAiD; or forgo effective, medically appropriate symptom control in order to maintain the capacity required in order to access MAiD. This is clinically and ethically indefensible. Under the law, is it necessary?
The interpretive uncertainty here is what constitutes “imminent” loss of capacity to provide informed consent. One interpretation of “imminent” is arising naturally from an illness, disease or disability. Another is that the loss of capacity is arising naturally either from the illness, disease or disability or from proper medical treatment of it (including sedation or other incapacitating levels of pain medication).
Loss of capacity to provide informed consent may be regarded as imminent when it is caused by the underlying condition alone or in concert with other natural conditions; or when the patient is at risk of permanent loss of capacity to consent to MAiD while under sedation or other medication required to alleviate suffering.
This proposed interpretation would address situations in which it appears that the only option for some patients who wish to access MAiD is to refuse ethically and medically appropriate symptom relief in order to be sure to have decision-making capacity at the end of the 10-day waiting period.
We emphasize that this interpretation would not allow the triggering of the exception to the 10-day waiting period in any and all cases. In other words, it is not just a way to circumvent the 10-day rule for everyone who asks for sedation or pain relief. The exception would be triggered only when the patient’s condition is such that the patient requires incapacitating levels of medication to alleviate suffering and risks permanent loss of capacity (and therefore permanent loss of the opportunity to access MAiD) while under that medication.
There are precedents in other areas of end-of-life practice that allow treatment decisions to determine important ethical and legal boundaries rather than insisting that they be determined solely by biological disease processes. For example, in the practice of organ donation after cardio-circulatory death, a decision is taken to withdraw life-sustaining ventilation from a patient. When the patient’s heart stops as a result of the withdrawal of ventilation, a period of 2, 5, 10 or 20 minutes of “hands-off” time is observed before death is declared; how long varies by country (Downie et al. 2009). During this time and even after death declaration, the patient could quite possibly be resuscitated. Despite this, the decision not to resuscitate allows the patient to be declared dead due to the irreversible cessation of cardio-respiratory function. In these cases, the refusal of resuscitation, rather than the biological condition of the patient, makes the cardio-respiratory function irreversible. The fact that the law prohibits attempting resuscitation on a patient against their wishes creates a state of legal irreversibility that is taken to be sufficient.
Similarly, in the case of MAiD, the ethically and medically appropriate treatment decision to apply and maintain sedation or other symptom control is what makes a person’s incapacity imminent, rather than the biological disease processes. If clinically indicated imminence of loss of capacity were taken to operate in the MAiD assessment just as legal irreversibility does in the determination of death, we could avoid the unacceptable dilemmas facing some MAiD requesters.
The legislation does not specifically exclude persons whose sole underlying condition is a mental illness from access to MAiD. The eligibility criteria (see sections 3.1 to 3.4 above) make no mention of mental illness or, indeed, any specific conditions. However, some of the eligibility criteria might have the effect of excluding persons with mental illness and no other condition. In addition, two passages in Bill C-14 mention “requests where mental illness is the sole underlying medical condition.”51 They might be taken to imply that such requests are excluded from eligibility for MAiD.
Are people whose sole underlying medical condition is a mental illness excluded from eligibility for MAiD? Or can they be eligible if they meet all of the criteria set out in the legislation?52
Despite the lack of explicit language in the Criminal Code excluding people whose sole condition is a mental health condition from MAiD if they satisfy all of the eligibility criteria, some health authorities have taken the position that MAiD is not permitted where mental illness is the sole underlying medical condition. For example, the Winnipeg Regional Health Authority (2016) has stated that “MAiD is not permitted: where mental illness is the sole underlying medical condition.” The Nova Scotia Health Authority (2016) made a similar statement.
It also appears that persons with mental illness as the sole underlying condition are being denied access to MAiD whether or not they meet the eligibility criteria: “Of the 18 patients that were denied, five of them had a mental illness as their underlying condition, and that precludes them from accessing…the service” (“Winnipeg Health Authority” 2017).
Persons with mental illness, whether as the sole underlying medical condition or as a comorbidity, are not automatically excluded from access to MAiD. They are eligible under the law if they meet all of the eligibility criteria set out in s.241.2. Some persons with mental illness as their sole underlying medical condition may meet the criteria.
As noted, the legislation’s eligibility criteria for access to MAiD do not explicitly exclude cases in which mental illness is the sole underlying condition. While many people in this situation will fail to meet one or more of the eligibility criteria, a small number will be able to meet them all, for these reasons:
Nevertheless, some have concluded that people whose sole underlying condition is a mental illness are always ineligible. Some have cited the provisions in Bill C-14 that call for “non-legislative measures” to explore “situations giving rise to requests by mature minors, advance requests and requests where mental illness is the sole underlying medical condition”53 and “independent reviews of issues relating to requests by mature minors for medical assistance in dying, to advance requests and to requests where mental illness is the sole underlying medical condition.”54 The inference some suggest we should draw is that since mature minors55 and advance requests56 are explicitly excluded from eligibility, requests from persons with mental illness as the sole underlying medical condition are also excluded, because they are included in lists with those other two categories in the passages quoted here.
A contrary interpretation is of course possible. The lists are not described in the legislation as excluded categories. Rather, they are lists of situations raising issues that the legislature felt required exploration through independent review. In making these lists, the legislature may have had in mind that many (but not all) people with mental illness as their sole underlying condition may be unable to meet all of the eligibility criteria (and so they are effectively, if not explicitly, excluded); the legislature may have intended these cases to be considered along with the other two explicitly excluded groups. It seems logical that, if the drafters had intended to exclude all individuals whose sole underlying medical condition is a mental illness, they would have done so in the sections of the legislation that actually establish the eligibility criteria — but they did not.
Looking at policy intent, some see signs that the government meant to exclude persons with mental illness as the sole underlying medical condition. They point, for example, to the government website that originally told the public, “You are not eligible for this service if: you are suffering only from a mental illness” (Canada 2017a).57 They also point to comments made by the government at the time of the parliamentary debates on C-14.58 However, around the same time, the government indicated that the legislation did not exclude persons whose sole underlying condition was a mental illness, as they would be able to apply and receive MAiD if they satisfied the same eligibility criteria as others.59
In 2017, when formally asked about the policy intent of the legislation, Minister Wilson-Raybould confirmed that the government did not intend to exclude from eligibility those whose sole underlying medical condition was a mental illness:
In crafting the legislation, the Government intended to make medical assistance in dying available to all competent adults who are in decline and approaching the end of their natural lives, in order that they may have the choice of a peaceful death instead of a painful, prolonged, or frightening one. Our policy was to treat the specific reasons underpinning the final stage of an individual’s life as irrelevant to his or her eligibility.
I wish to be clear that the Government’s intention with this legislation was and remains that a person who meets all of the eligibility criteria may receive medical assistance in dying. As long as all of the criteria are satisfied, the legislation is silent with respect to whether a person’s medical condition is a mental illness.
In addition, in commenting on the independent review required by the legislation, the Minister gave an example of a person with a mental illness as their sole underlying medical condition who could nonetheless qualify for MAiD:
The review is not intended to focus on cases where an individual with mental illness, in combination with other medical circumstances, would already qualify for medical assistance in dying, such as a competent person with incurable cancer in an advanced state of decline who also experiences mental illness, or where a mental illness, such as an eating disorder, is at such an advanced stage that the individual will die as a result.60
It should be noted here, before closing, that few patients with mental illness as the sole underlying medical condition will meet all of the eligibility criteria. In particular, few will meet the criterion of their natural death being “reasonably foreseeable.” Some, but not all, will fail to meet the legal standard of mental capacity. For some, their condition may be curable and their suffering remediable. However, some may meet all the criteria and, if they do, then the legislation does not otherwise exclude them.
It should also be noted that good clinical practice requires that medical or nurse practitioners assessing persons whose sole underlying medical condition is a mental illness ensure that they have the professional competencies required for the assessment of capacity and of the eligibility criteria (in particular, irremediability of suffering) in such cases.
Uncertainty about the meaning of specific terms in Canadian MAiD legislation puts Canadians at risk in a number of ways. Eligibility for MAiD may be determined too broadly or too narrowly, and there may be arbitrary inequality of access when different MAiD assessors and providers interpret the law differently. During the 10-day waiting period, some patients may avoid ethically and medically appropriate pain control in order to try to maintain decision-making capacity. The uncertainty may also result in a chilling effect on medical and nurse practitioners’ willingness to provide MAiD.
Although only a court can issue definitive interpretations of the law, there is room for governmental, regulatory and nongovernmental organizations to adopt, endorse and/or disseminate the proposed interpretations in this report (collected in box 3). This would help to move the public discussion toward potential consensus on the meaning of the terms in the legislation.
We therefore invite Canadians to join us in calling for the following:
Jocelyn Downie is a member of the Canadian Council of Academies Expert Panel on Medical Assistance in Dying, and she was a member of the Royal Society of Canada Expert Panel on Physician Assisted Dying, the Provincial-Territorial Expert Advisory Group on Physician Assisted Dying, and the pro bono legal team for the plaintiffs in Carter v. Canada. She is a university research professor in the faculties of law and medicine at Dalhousie University, a faculty member of the Dalhousie Health Law Institute, and an adjunct professor at the Australian Centre for Health Law Research. She is a member of the Order of Canada and a Fellow of the Royal Society of Canada, the Canadian Academy of Health Sciences, and the Pierre Elliott Trudeau Foundation.
Jennifer A. Chandler is a member of the Canadian Council of Academies Expert Panel on Medical Assistance in Dying. She is the Bertram Loeb Research Chair and a professor at the Centre for Health Law, Policy and Ethics, Faculty of Law, University of Ottawa.
The authors are deeply indebted to the participants of the meeting we convened in August 2017 under the Chatham House Rule. Their generous and constructive engagement with the drafts of this report and their commitment to a collaborative process aimed at increasing clarity with respect to the meaning of Canada’s MAiD legislation has been extraordinary. The meeting was made possible by the Pierre Elliott Trudeau Foundation fellowship held by Jocelyn Downie. The authors are also grateful to other experts who generously provided sometimes challenging and always helpful feedback on earlier drafts of this report.
To cite this study: Downie, Jocelyn and Jennifer A. Chandler. Interpreting Canada’s Medical Assistance in Dying Legislation. IRPP Report (March 2018). Montreal: Institute for Research on Public Policy. DOI: https://doi.org/10.26070/efpr-9034
Cecile Bensimon, PhD, Director, Ethics and Professional Affairs, Canadian Medical Association
Shelley Birenbaum, JD, MSW, MBE, President and Counsel at Shelley R. Birenbaum Professional Corporation
Jennifer Chandler, BSc, LLB, LLM, Bertram Loeb Research Chair, Professor of Law, University of Ottawa
Pierre Deschamps, LScR, BCL, CM, AdE
Jocelyn Downie, BA, MA, MLitt, LLB, LLM, SJD, FRSC, FCAHS, University Research Professor, Faculties of Law and Medicine, Dalhousie University
Jennifer Gibson, BSc, BA, MA, PhD, Director, Joint Centre for Bioethics, Sun Life Financial Chair in Bioethics, University of Toronto
Gus Grant, AB, LLB, MD, CCFP, Registrar and CEO, College of Physicians & Surgeons of Nova Scotia
Stefanie Green, BSc, MDCM, CCFP, President, Canadian Association of MAID Assessors and Providers
Tim Holland, MD, CCFP (EM), Chair, Committee on Ethics, Canadian Medical Association
April Negus, BScN, RN, MN, Specialty Nurse Practitioner Geriatric Medicine
Carolyn Pullen, BScN, RN, PhD, Chief, Policy and Programs, Canadian Nurses Association
Eric Wasylenko, MD, CCFP (PC), BSc, MHSc (Bioethics), Clinical Associate Professor, Cumming School of Medicine, University of Calgary; Clinical Lecturer, John Dossetor Health Ethics Centre, University of Alberta; Medical Director, Health System Ethics and Policy; Health Quality Council of Alberta
Note: The people listed do not necessarily endorse all statements in this report.
ALS Association. n.d. “Who Gets ALS?” Accessed January 19, 2018. webma.alsa.org/site/Page Server/?pagename=MA_1_WhoGets.html
British Columbia. 2016. Ministry of Justice, Criminal Justice Branch. Crown Counsel Policy Manual: “Medical Assistance in Dying and Related Prosecutions.” No. 56880-00, MED 2, October 28. Accessed January 19, 2018. https://www2.gov.bc.ca/assets/gov/law-crime-and-justice/criminal-justice/prosecution-service/crown-counsel-policy-manual/med2-medical-assist ance-dying.pdf
Canada. 2016a. Department of Justice Canada. “Glossary.” Accessed January 19, 2018. www.justice.gc.ca/eng/cj-jp/ad-am/glos.html
———. 2016b. Department of Justice Canada. Legislative Background: Medical Assistance in Dying (Bill C-14, as Assented to on June 17, 2016). Accessed January 19, 2018. www.justice.gc.ca/eng/rp-pr/other-autre/adra-amsr/index.html
———. 2017a. “Medical Assistance in Dying.” Accessed January 19, 2018. https://www.canada.ca/en/health-canada/services/medical-assistance-dying.html
———. 2017b. “Monitoring of Medical Assistance in Dying Regulations.” Regulatory Impact Analysis Statement. Canada Gazette 1, vol. 151, December 16. Accessed January 19, 2018. https://www.gazette.gc.ca/rp-pr/p1/2017/2017-12-16/html/reg6-eng.html
———. 2017c. Health Canada. “2nd Interim Report on Medical Assistance in Dying in Canada,” October. Accessed January 19, 2018. https://www.canada.ca/en/health-canada/services/publications/health-system-services/medical-assistance-dying-interim-report-sep-2017.html
Canadian Association of MAID Assessors and Providers. 2017. “Resources.” Accessed January 19, 2018. https://camapcanada.ca/resources.html
Canadian Medical Association. n.d. “Education on Medical Assistance in Dying.” Accessed January 21, 2018. https://www.cma.ca/En/Pages/education-eol-care-medical-assistance-dying.aspx
Canadian Nurses Association. 2017. “National Nursing Framework on Medical Assistance in Dying in Canada.” Accessed January 19, 2018. www.cna-aiic.ca/~/media/cna/page-content/pdf-en/cna-national-nursing-framework-on-maid.pdf?la=en
CBC News. 2017. “Ontario to Limit Criminal Prosecutions of HIV-Positive People Who Don’t Disclose Status.” December 1. Accessed January 19, 2018. www.cbc.ca/news/canada/toronto/ontario-limit-hiv-positive-people-criminal-1.4429208
Chatham House. n.d. “Chatham House Rule.” Accessed January 19, 2018. https://www.chatham house.org/about/chatham-house-rule?gclid=CNfEzPy0xdYCFdmPswodwzgIEQ
College of Physicians & Surgeons of Nova Scotia. 2017. “Professional Standard Regarding Medical Assistance in Dying.” Accessed January 19, 2018. https://cpsnc.ns.ca/wp.-content/uploads/2016/06/Professional-Standard-regarding-Medical-Assistance-in-Dying.pdf
Council of Canadian Academies. n.d. “Assessments in Progress: Medical Assistance in Dying.” Accessed January 19, 2018. https://www.scienceadvice.ca/en/assessments/in-progress/med ical-assistance-dying.aspx
Downie, J. 2018. “Hasty Change to Assisted Dying Bill a Serious Error.” Policy Options (January 2018). Accessed February 20, 2018. https://policyoptions.irpp.org/magazines/january-2018/hasty-change-to-assisted-dying-bill-a-serious-error/
Downie, J. and Chandler, J.A. 2017. “Interpreting Canada’s Medical Assistance in Dying Legislation” SSRN. Accessed February 23, 2018. https://ssrn.com/abstract=2976521
Downie, J., and J. Dembo. 2016. “Medical Assistance in Dying and Mental Illness Under the New Canadian Law.” Journal of Ethics in Mental Health (Open Volume). Accessed January 19, 2018. https://www.camapcanada.ca/dd2016.pdf
Downie, J., M Kutcher, C. Rajotte, and A. Shea. 2009. “Eligibility for Organ Donation: A Medico-Legal Perspective on Defining and Determining Death.” Canadian Journal of Anesthesia 56: 851.
Downie, J., and K. Scallion. Forthcoming. “Foreseeably Unclear: The Meaning of the ‘Reasonably Foreseeable’ Criterion for Access to Medical Assistance in Dying in Canada.” Dalhousie Law Journal. Available online at SSRN. Accessed February 27, 2018. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3126871
Downie, J., and B. White. 2012. “Prosecutorial Discretion in Assisted Dying in Canada: A Proposal for Changing Guidelines.” McGill Journal of Law and Health 6 (2): 113-72.
Dying With Dignity Canada. n.d. “Know Your Rights.” Accessed February 20, 2018. https://www.dyingwithdignity.ca/know_your_rights
House of Commons. 2016a. Debates of the House of Commons. 42nd Parliament, 1st session, vol. 148, no. 45, April 22.
———. 2016b. Debates of the House of Commons. 42nd Parliament, 1st session, vol. 148,
no. 46, May 2.
———. 2016c. Debates of the House of Commons. 42nd Parliament, 1st session, vol. 148, no. 62, May 31.
———. 2016d. Debates of the House of Commons. 42nd Parliament, 1st session, vol. 148, no. 74, June 16.
House of Commons Standing Committee on Justice and Human Rights. 2016. Committee Evidence, 42nd Parliament, 1st Session, no. 10, May 2.
Jutai, J.W., S. Bhogal, N. Foley, and M. Speechley. 2003. “Treatment of Visual Perceptual Disorders Post Stroke.” Accessed January 20, 2018. https://www.researchgate.net/publication/9885596_Treatment_of_Visual_Perceptual_Disorders_Post_Stroke
Knuti, K.A., P. Amrein, B. Chabner, T. Lynch Jr., and R. Penson. 2002. “Faith, Identity, and Leukemia: When Blood Products Are Not an Option.” The Oncologist, August 7 (4): 371-80. Accessed January 20, 2018. theoncologist.alphamedpress.org/content/7/4/371.full
Lekoubou, A., E. Gleichgerrcht, K. McGrattan, D. Bachman, R. J. Adams and L. Bonilha 2015. “Aphasia in Multilingual Individuals: The Importance of Bedside Premorbid Language Proficiency Assessment.” eNeurologicalSci 1 (1): 1.
Martel, L. 2015. “Mortality: Overview, 2010 and 2011.” Report on the Demographic Situation in Canada. Catalogue 91-209-X, November 30. Ottawa: Statistics Canada.
Nova Scotia Health Authority. 2016. “Medical Assistance in Dying: Frequently Asked Questions for Physicians & Nurse Practitioners,” July 6. Accessed January 20, 2018. www.nshealth.ca/sites/nshealth.ca/files/faq_physiciansnps_2016_07_06.pdf
Rockwood, K., X. Song, C. MacKnight, and H. Bergman et al. 2005. “A Global Clinical Measure of Fitness and Frailty in Elderly People” Canadian Medical Association Journal 173 (5): 489-5.
Roussy, K. 2017. “Parkinson’s Patient Forced to Battle Bureaucracy Around Assisted Death.” CBC News, December 14. Accessed January 20, 2018. www.cbc.ca/news/health/parkinson-s-as sisted-death-canada-doctors-maid-1.4416392
Senate. 2016a. Debates of the Senate. 42nd Parliament, 1st session, vol. 150, no. 41, June 1. Accessed February 27, 2018. https://sencanada.ca/en/content/sen/chamber/421/debates/041db_2016-06-01-e#2
——— 2016b. Debates of the Senate. 42nd Parliament, 1st session, vol. 150, no. 52, June 17. Accessed February 27, 2018. https://sencanada.ca/en/content/sen/chamber/421/debates/052db_2016-06-17-e
Standing Senate Committee on Legal and Constitutional Affairs. 2016a. Proceedings. 42nd Parliament, 1st session, issue no. 8, “Evidence,” May 4. https://sencanada.ca/en/Content/SEN/Committee/421/lcjc/08ev-52539-e
———. 2016b. Proceedings. 42nd Parliament, 1st session, issue no. 8, “Evidence,” May 5. Accessed January 20, 2018. https://sencanada.ca/en/Content/SEN/Committee/421/lcjc/08ev-52552-e
———. 2016c. Proceedings. 42nd Parliament, 1st session, issue no. 10, “Evidence,” June 6. Accessed January 20, 2018. https://sencanada.ca/en/Content/SEN/Committee/421/lcjc/10ev-52666
VPS-NPV. 2017. “Understanding the Vulnerable Persons Standard.” Accessed January 20, 2018. www.vps-npv.ca/read-the-standard-20
Wilson-Raybould, J. 2017. Minister of Justice and Attorney General of Canada. Letter. April 19. https://eol.law.dal.ca/wp-content/uploads/2017/11/Letter-from-the-Minister.pdf
“Winnipeg Health Authority Doubles Number of Doctors Working in Assisted Dying Program.” Toronto Star, January 10, 2017. Accessed January 20, 2018. https://www.thestar.com/news/canada/2017/01/10/winnipeg-health-authority-doubles-number-of-doctors-working-in-assisted-dying-program.html
Winnipeg Regional Health Authority. 2016. “Medical Assistance in Dying.” Standards of Practice. Accessed January 20, 2018. https://www.wrha.mb.ca/maid/health_professionals_standards.html
Montreal – Uncertainty about the meanings of specific terms in the Canadian medical assistance in dying (MAiD) legislation must be addressed, says a new report from the Institute for Research on Public Policy.
The federal government passed legislation in June 2016 that allows eligible Canadians to request medical assistance in dying. But that legislation contains many terms that must be better defined, say the authors Jocelyn Downie (Dalhousie University) and Jennifer A. Chandler (University of Ottawa).
Interpretive uncertainty concerning Bill C-14 puts Canadians at risk in a number of ways, they say. “Individuals who should have access may be denied, while others may be given access who should not. This uncertainty may also result in a chilling effect on medical and nurse practitioners’ willingness to provide MAiD.” Additionally, serious problems arise in relation to the 10-day waiting period, where some patients may avoid ethically and medically appropriate pain control in order to maintain decision-making capacity.
Downie and Chandler identify the most problematic phrases in Bill C-14, which urgently need clarification, such as “intolerable suffering” or “an advanced state of irreversible decline.” They also address the most unclear and controversial phrase of all – “natural death has become reasonably foreseeable.” Does it mean that eligibility is limited to fatal conditions? Do patients have to be “terminally ill” or “at the end of life”? Does death have to be in the “not too distant future”? If so, how distant is too distant?
Downie and Chandler conclude by inviting all responsible authorities to adopt, endorse and/or disseminate the proposed interpretations in the report in an effort to provide much needed guidance to patients and health care practitioners and help build public consensus on these important matters. Among others, the authors suggest the Minister of Justice and Attorney General of Canada publicly state that the proposed interpretations are (or are not) consistent with the intentions of the legislation.
Interpreting Canada’s Medical Assistance in Dying (MAiD) Legislation, by Jocelyn Downie and Jennifer A. Chandler, can be downloaded from the Institute’s website (irpp.org).
______________________________________________________________________________
The Institute for Research on Public Policy is an independent, national, bilingual, not-for-profit organization based in Montreal. To receive updates from the IRPP, please subscribe to our e-mail list.
Media contact: Shirley Cardenas tel. 514-594-6877 scardenas@nullirpp.org
Medical assistance in dying has been legal in Canada for nearly two years, but confusion around how to interpret the legislation persists.
When the federal government passed Bill C-14 in June 2016, reactions to the law were immediate and vociferous. Some felt that it was too permissive, while others felt that it was too restrictive. It was widely noted that the meaning of some of the legislation’s key terms and phrases was unclear. Questions were raised about specific terms, such as “intolerable suffering” or “an advanced state of irreversible decline.” Perhaps most controversially, does the “reasonably foreseeable natural death” criterion mean that eligibility is limited to those with fatal conditions or who are “terminally ill” or “at the end of life” or whose death is “in the not too distant future”?
Ongoing uncertainty around these terms is putting Canadians at risk in a number of ways. Too narrow an interpretation could mean people who should have access may be denied MAID; too broad an interpretation could mean some people may be given access who should not. Indeed, two persons in the same circumstances may be treated differently simply because their MAID assessors and providers interpret the law differently.
Other consequences are possible, too. For example, in response to particular interpretations of the law that suggest no other option, some patients may forgo drugs needed for effective pain control and remain in a state of intolerable suffering to keep the necessary level of decision-making capacity to reiterate their request for MAID at the time of administration. In addition, interpretive uncertainty may also raise concerns about potential criminal liability, producing a chilling effect on medical and nurse practitioners’ willingness to provide MAID.
How can we avoid these consequences? Once a piece of legislation is in force, only the courts can definitively interpret it. Unfortunately, seeking clarification through litigation is prohibitively expensive and time consuming. Few people denied access to MAID because of issues of interpretation would be in a position to seek assistance from the courts.
Until the courts step in with definitive interpretations, there are nevertheless steps that can be taken to mitigate the problems mentioned above. Indeed, in the shorter term, there are instruments and avenues available to reduce uncertainty and confusion among patients and health care providers. We outline some of them in our recent report for the Institute for Research on Public Policy, where we determine the most defensible interpretations of the legislation, using the tools of statutory interpretation supported by the relevant clinical and other forms of expertise.
We call on those who have the responsibility and authority to provide interpretive guidance to health-care practitioners and patients to adopt, endorse and/or disseminate these proposed interpretations in order to build consensus on the meaning of the terms of the legislation. This is a task that concerns governments, directors of public prosecution and attorneys general, professional regulators, health authorities, professional liability protection providers, professional associations and civil society groups.
In particular, we invite Canadians to join us in calling for:
• The Minister of Justice and Attorney General of Canada to publicly state that the proposed interpretations are consistent (or not inconsistent) with the government’s intentions when crafting the legislation.
• The federal government to reflect the proposed interpretations in an update to the glossary that the Department of Justice posted on the internet to accompany the legislation when it was introduced and in the regulations establishing the federal monitoring system.
• The directors of public prosecution and attorneys general in each province and territory to reflect the proposed interpretations in guidelines for the exercise of prosecutorial discretion in the context of MAID.
Although 1,982 Canadians accessed MAID in the legislation’s first year, confusion remains around some of its key terms and clarity is required. Together we must move the public discussion toward a potential consensus. It is time for those who can help to clarify the meanings to do so.
Jocelyn Downie is a professor at the Schulich School of Law, Faculty of Medicine, and Health Law Institute at Dalhousie University. Jennifer Chandler is a professor in the Centre for Health Law, Policy and Ethics at the Faculty of Law at the University of Ottawa.
The federal government passed legislation in June 2016 that allows eligible Canadians to request medical assistance in dying. But that legislation contains many terms that continue to generate uncertainty and confusion among patients and health care providers, and require clarification, say Jocelyn Downie and Jennifer Chandler in a recent report from the Institute for Research on Public Policy. In this webinar, the authors discuss some of the interpretative difficulties posed by the current legislation in determining eligibility and the solutions they propose to bring greater clarity to the process.
Video
Presentation
New research by Jocelyn Downie and Jennifer Chandler explores interpreting Canada’s Medical Assistance in Dying legislation.




