
Long-Term Care Financing: What’s Fair and Sustainable?
Frances Woolley

Seniors are the heaviest users of prescriptions medicines in Canada. On average, two-thirds take 5 or more prescriptions drugs over the course of a year and one-quarter take 10 or more. It is estimated that as much as half of the medications given to seniors are taken incorrectly or are overprescribed, increasing the likelihood of adverse drug reactions and interactions. Moreover, many drugs prescribed to seniors either have not been adequately studied for this age group or have not been formally approved for the conditions they are being prescribed to treat. Indeed, clinical trials often exclude not only older people, but also people of all ages who take a combination of medications. As a result, certain medications are prescribed to seniors without any evidence they are safe and effective for them, and in some cases even when they are known to present a possible risk (antipsychotics prescribed to patients with dementia, for example).
In this study, Nicole Bernier examines the problem and consequences of unsafe and inappropriate use of prescription drugs by seniors and presents possible solutions. She observes that governments have relied heavily on the voluntary efforts of professional groups and patients to address the issue, when they could use legislation and financial instruments to much greater effect.
Bernier documents many collaborative initiatives undertaken by professionals, advocacy groups and health authorities to provide information and educational resources, reallocate roles and responsibilities, and promote innovation. She argues that while such initiatives are valuable, their overall effectiveness is limited, because they address only narrow aspects of a much bigger problem. In her view, improving prescription drug safety among seniors will require systemic change, and hence leadership and engagement, from Health Canada, provincial and territorial health ministries, and local health authorities.
What is needed, she maintains, is a comprehensive national strategy. Building on the 2015 recommendations of the Senate Committee on Social Affairs, Science and Technology, such a strategy would entail a more proactive role for Health Canada. It would include revising the drug approval process, monitoring newly marketed drugs prescribed to seniors, improving reporting on adverse drug reactions, and encouraging independent research into off-label prescription drug use. In addition, provinces and territories would be called upon to update their prescribing guidelines regularly, require medication reviews, and provide coverage for effective nondrug therapies. Health authorities would also ensure that professionals have access to clinical decision-making tools, as well as accurate and comprehensive information on patients’ medical histories, in order to improve prescribing practices overall.
When it comes to seniors’ health, Bernier concludes, prescribing practices are too often based on little or no evidence, and as a result can be inappropriate and even dangerous. Much more can and should be done to address this serious health issue for our aging population.
Seniors’ use of prescription medicines presents significant challenges, with implications for policy-makers, clinicians and the general public. Among the concerns are the quality and safety of health care for many seniors and the inefficient use of Canada’s public resources. Seniors aged 65 and over are the heaviest users of prescription medicines. The vast majority of them are using prescription drugs (Rotermann et al. 2014, 5). Two-thirds take 5 or more prescription drugs, and a quarter take 10 or more drugs, on average, over the course of a year (CIHI 2014, 22). Experts have pointed to increased drug utilization as the biggest driver of drug spending in Canada for some years (CIHI 2014, 11). In 2013, $419 million was spent on potentially inappropriate medication1 outside of hospital settings, in six provinces (Morgan et al. 2016).
But safety issues are increasingly salient. It is estimated that half of the medication given to seniors is not taken correctly or is prescribed in an excessive manner. When medications are not appropriately prescribed and supervised, they can cause adverse drug reactions (ADRs) such as unsteadiness, confusion, delirium, depression and dependence (Chief Public Health Officer 2010, 30-1). Seniors are five times more likely than younger Canadians to be hospitalized as a result of an adverse drug reaction (Senate of Canada 2014b, 15). In 2011, over 27,000 Canadian seniors — that is, one in 200 — had an ADR-related hospitalization. An estimated 2.8 percent of all hospitalizations among seniors are attributable to ADRs from medications (CIHI 2013, 15). The likelihood of being hospitalized for an ADR increases with age; for instance, seniors aged 85 and older are 1.7 times more likely to be hospitalized for an ADR than those aged 65 to 74 (CIHI 2013, 13).
Many people might be surprised to learn that in Canada a large proportion of the medications administered to at-risk groups — seniors (aged 65 and older) as well as children and pregnant and nursing women — have never been adequately studied or formally approved for the conditions they are commonly prescribed to treat. Three out of four drugs prescribed to patients under 18 in this country are not approved for patients in that age group or are prescribed for a condition other than that for which they were approved (Senate of Canada 2014a, 5). In addition, some medications are prescribed to patients even when they are known to present a potential risk to the user. Such practices have been unveiled in part by ongoing coverage of drug safety scandals in recent years. Journalists have brought to light the widespread off-label use of antipsychotic drugs for patients with dementia in residential care — a practice that increases the risk of mortality (Stueck 2012; Bruser 2014; Walkom 2016). These scandals are only the tip of the iceberg.
In this study I examine the problem and the consequences of unsafe and inappropriate use of prescription drugs by seniors, as well as potential solutions. While health professionals, patients and other stakeholders can all contribute in some capacity to more appropriate medication use among the elderly, the scope and scale of the problem are such that leadership and engagement from Health Canada, provincial and territorial health ministries, and regional and local health authorities are essential to bring about the systemic changes required.
Clinical evidence on the effectiveness and safety of treating seniors with medication is hard to come by. One reason is that the elderly are underrepresented in clinical drug trials. Indeed, for most of the medications they prescribe to older patients, doctors have to rely on evidence from trials that exclude seniors (Kwan and Farrell 2014; CIHI 2011, 60; Duerden, Avery and Payne 2013, 29). And even when clinical evidence indicates that a drug is inappropriate for older patients or may be harmful to them, that evidence is too often overlooked (Senate of Canada 2014a). This gap in clinical evidence and the lack of attention to the little evidence there is can be detrimental to the health and well-being of seniors.
Seniors face a higher risk of adverse drug reactions, in part because of physiological changes as we age that alter the way our bodies respond to medication (pharmacokinetics) and process them (pharmacodynamics). For instance, our kidneys and liver tend to lose functional ability and become less efficient in flushing out drugs (Patterson et al. 2014, 5; CIHI 2011, 60; Senate of Canada 2014a, 9).
When Health Canada approves a drug for sale, it specifies “the population for whom the drug can be prescribed, the indication(s) the drug can treat, and the dosage(s) that can be admini-stered” (Senate of Canada 2014a, 3). Across the country, however, drugs are often prescribed off-label: that is, to subgroups of the population, for indications or at dosages that do not correspond to the approved criteria. This means that in certain cases doctors are prescribing drugs to older adults (or children and pregnant and nursing women) even though there is no evidence that they are safe and effective for these patients (Senate of Canada 2014a, 5).
Off-label use is not prohibited as such, and sometimes it can be useful: for instance, in treating rare disorders. But rare disorders account for only a tiny proportion of Canada’s off-label prescriptions, which are very common. For children, for instance, 75 percent of medications are prescribed off-label (Senate of Canada 2014a, 5). Data on off-label use by seniors are limited, but a study found that in Quebec, one in nine prescription drugs (11 percent) is given for an off-label indication (Eguale et al. 2012, cited in Senate of Canada 2014a, 4). The problem with drugs prescribed off-label to seniors is that the vast majority (79 percent) of these prescriptions are not supported by strong scientific evidence of efficacy, as would be provided by at least one randomized, controlled clinical trial.
Evidence of a drug’s inappropriateness for seniors is too often ignored in prescribing practices. Drugs are considered to be potentially inappropriate when they expose seniors to an elevated risk of adverse effects, when they are not efficacious for them or when safer alternatives are available (CIHI 2014, 25). In 1991, Mark H. Beers developed a list of potentially inappropriate drugs to be avoided in older adults, which is regularly updated by the American Geriatrics Society. In 2012, 38.9 percent of Canadian seniors used a drug on the Beers list, and 12.4 percent of seniors used two or more such drugs. In addition, 22.4 percent of seniors used at least one drug from the Beers list chronically (CIHI 2014, 26).2
Seniors living in institutions are particularly exposed to the risk of using potentially inappropriate drugs, in part because the rate and quantity of drug consumption among this group are very high. When surveyed, almost all seniors living in institutions (97 percent) reported having used at least one medication (prescription or over the counter) in the two days preceding the interview, and over half (53 percent) reported having used five or more (Chief Public Health Officer 2010, 30). There is growing evidence that some drugs prescribed in these settings are used not to treat medical symptoms but for discipline or staff’s convenience. For instance, drugs may be used as chemical restraints for residents who are agitated, have a tendency to wander or display aggressive behaviours.3 The practice of sedating residents so they are no longer intrusive or distracting in their behaviour has a name: it is called “snowing” by some nursing home staff (Seniors at Risk 2012).
Antipsychotics are widely used in nursing homes. In 2014, some 39 percent of Canadians living in long-term-care facilities received at least one antipsychotic (CIHI 2016, 14). In British Columbia, only 4 percent of seniors in residential care have a diagnosis of a psychiatric disorder, but 34 percent are on antipsychotic medications (British Columbia 2015). Across Canada, older nursing home residents are nine times more likely to be given antipsychotics than their counterparts who live in the community (CIHI 2014).
Drug labels and several warnings issued by Health Canada make it clear that antipsychotics can be dangerous for patients with dementia — many of whom live in nursing homes — and that their use should be restricted to addressing short-term problems. When inappropriately prescribed, these drugs may increase the risk of side effects such as “sedation, a sudden drop in blood pressure, falls, fractures, stroke and death” (CIHI 2016, 13).
Another significant gap in evidence for safety and efficacy arises from the practice of studying drugs in isolation, whereas seniors frequently use multiple medications. Clinical trials often exclude not only older people but also people who take a combination of medicines, so they may fail to identify adverse drug reactions and drug interactions, especially in older patients (Duerden, Avery and Payne 2013, 29; Kwan and Farrell 2014; CIHI 2011, 60).
The intensity of prescription drug use tends to increase when people age, partly because older people are more likely to have more than one health condition. Three out of four Canadian seniors have been diagnosed with at least one chronic condition (such as hypertension, arthritis, cancer, diabetes, chronic obstructive pulmonary disease), and one in four has three or more such conditions (McPherson et al. 2012, 15-18). In 2014, two out of three seniors (66.1 percent) took 5 or more drugs; 28.0 percent took 10 or more drugs; and 9.3 percent took 15 or more drugs (National Prescription Drug Utilization Information System Database, Canadian Institute for Health Information).
Taking multiple drugs may be desirable for some elderly patients. Under the right conditions; combining drugs can improve many older patients’ outcomes (Duerden, Avery and Payne 2013, 4). When it is appropriately prescribed and supervised, “pharmaceutical therapy can prolong life, reduce suffering and increase quality of life for seniors” (Chief Public Health Officer 2010, 30). But -multiple drug use can be risky for seniors because, as stated earlier, they are more susceptible to adverse drug reactions (Millar 1998, 11; Ramage-Morin 2009, 40; Reason et al. 2012, 431). Polypharmacy — that is, taking five or more medications — can create dangerous drug interactions and increases the risk of frailty, disability, poor treatment adherence, hospitalization and mortality. Patients are also more likely to experience falls, cognitive difficulties, decreased awareness, unsteadiness, dizziness and excessive sedation (CIHI 2013, 12; Gamble et al. 2014, 190).
The dangers of polypharmacy for seniors are seen in doctors’ offices and hospitals. The more medications they consume, the more likely seniors are to require urgent medical attention or go to emergency departments. A recent study found that 12 percent of Canadian seniors who take 5 or more medications have experienced a side effect requiring medical attention, as compared with 5 percent of those using only 1 or 2 medications. For each additional medication, there is a 2 percent increase in the likelihood of visiting the emergency department or being hospitalized (Allin, Rudoler and Laporte 2015, 13). In 2010, only 0.2 percent of seniors taking fewer than 5 drugs were hospitalized for an ADR, as compared with 2.2 percent of those who took 15 or more drugs (CIHI 2013, 11). Seniors taking 15 drugs or more were 6.4 times more likely to be hospitalized than those who took fewer than 5 drugs (CIHI 2013, 14).
The safety issues associated with seniors’ polypharmacy are not restricted to Canada and are not a new phenomenon either. As early as 1985, the World Health Organization launched a program called Rational Use of Medicines in an effort to reduce polypharmacy. In 1998, Statistics Canada published the article “Multiple Medication Use among Seniors” (Millar 1998), although it did not cover long-term residents of hospitals and residential care facilities, who are known to use more medications than seniors living in the community.
Polypharmacy trends and their evolution over the years cannot be easily traced. CIHI has published sporadic data on polypharmacy among seniors, based on the National Prescription Drug Utilization Information System. Quebec, Ontario, British Columbia and Alberta have databases containing the number of prescriptions, type of drugs and age groups of users, but no comprehensive portrait of polypharmacy trends has been published. Peer-reviewed journals tend to focus on specific aspects of the issue, such as financial costs to the health care system, the implications for professional practices and, to a lesser extent, the safety of patients.
What we do know is that the prevalence of multiple drug use has been rising significantly, from 54.7 percent of seniors using 5 prescription drugs or more in 2000 to 66.1 percent in 2014. In addition, the average number of prescription drugs taken by seniors rose from 5.9 to 7.4 over the same period (National Prescription Drug Utilization Information System Database, Canadian Institute for Health Information). In Ontario, the number of prescription claims and claims per person increased rapidly from 1997 to 2006, particularly for women aged 85 and older. For instance, prescriptions for preventive medications increased by 697 percent for lipid-lowering agents and by 2,347 percent in the case of prescriptions to prevent osteoporosis. The proportion of older patients who have prescriptions for more than 10 classes of medications almost tripled over this period (Bajcar et al. 2010).
A proper balance must be established between aggressively treating health conditions experienced by seniors and avoiding medication-related harm to them. Possible causes of the persistent gaps between evidence, warnings and prescribing practices include insufficient dissemination and use of existing knowledge about possible alternative therapies, patients dealing with multiple physicians and pharmacists, and communication problems between physicians and older adults, especially when patients have cognitive impairments that impede their ability to convey medication-related problems (Senate of Canada 2014a, 9; Chief Public Health Officer 2010, 31; Patterson et al. 2014, 4). Additional factors may include the promotion and marketing activities of the pharmaceutical industry (Steinman et al. 2006; Van Zee 2009; Spurling et al. 2010; Davison and Perron 2013) and clinical practice guidelines that are produced by authors who have conflicts of interest with the pharmaceutical industry (Neuman et al. 2011; Bindslev et al. 2013; Norris et al. 2013).
Since physicians are responsible for assessing patients’ conditions, making a diagnosis and prescribing drugs when necessary, they should make awareness of drug safety issues a top priority. Indeed, physicians are expected to weigh the risks and benefits of prescribing drugs and to act in their patients’ best interests (College of Physicians and Surgeons of Ontario 2016, 2-4). The reality, however, is that prescribing certain drugs to at-risk populations and monitoring them can be quite complex and difficult. To properly fulfill their role, physicians may need to have access to electronic medical records and clinical decision support tools. They may also need to consult with clinical pharmacists to help determine whether patients are taking medications that are no longer needed or that should be reduced in dosage.
That said, researchers are finding that professional awareness of drug safety issues is not as high as it should be. Emergency department doctors frequently fail to recognize ADRs (Hohl et al. 2010). A recent survey showed that in Quebec, fewer than 50 percent of pharmacists were aware of the prevalence of polypharmacy, inappropriate prescribing, drug-related hospitalizations or falls in the geriatric population. Only 48 percent of them were familiar with the Beers list of drugs to avoid in the elderly, and only 5.6 percent were aware that short-acting benzodiazepines should never be prescribed to older adults because of new evidence that they increase the risk of falls, hip fractures and cognitive impairment (Zou and Tannenbaum 2014).
Physicians and pharmacists may also have diverging views on which drugs should be removed from a patient’s drug regimen (Page et al. 2016). Deprescribing entails “an active review process that prompts the physician to consider which medications have lost their advantage in the risk-benefit trade-off, especially in patients with changing goals of care or limited life expectancy” (Frank 2014, 408). Deprescribing may lead to health complications, so professionals’ concerns about liability may become a disincentive for action.
In long-term-care homes, one commonly cited cause for the unsafe overmedication of many patients is the lack of accessible alternatives. For instance, staff may have limited tools, insufficient resources or inadequate training to deal with a dementia patient’s aggressive behaviour (Lexchin 2013). When system support, time and resources are lacking, physicians may be unable to recommend better ways to help patients and are left with drug prescription as the sole recourse to manage symptoms.
The Senate Committee on Social Affairs, Science and Technology conducted a three-year, four-phase study on prescription pharmaceuticals in Canada (Senate of Canada 2015). The committee examined the process of approving prescription pharmaceuticals, with a particular focus on clinical trials; the postapproval monitoring of prescription pharmaceuticals; the off-label use of prescription pharmaceuticals; and the unintended consequences of the use of prescription pharmaceuticals. While the committee did not focus on prescription drug use by seniors specifically, its deep and detailed examination of prescription drugs in Canada included the issues associated with at-risk groups of the population, for whom clinical data are scarce. The committee reports stressed that one of the main dangers with medications for seniors is that patients in at-risk groups are being prescribed drugs that have been tested only in the general population.
Moreover, there is no systematic process to record and monitor the effectiveness and safety of marketed drugs prescribed to seniors. For various reasons, ADR reports collected by Health Canada fail to provide a comprehensive review of the real-world safety and effectiveness of drugs already approved (Senate of Canada 2013, 12-13). Effectiveness studies conducted at several intervals (for instance, after 1, 5 and 10 years) following a drug’s release onto the market are necessary to determine how different groups (such as age and gender groups) respond to an approved drug. In 2009, the Canadian Institutes of Health Research and Health Canada launched the Drug Safety and Effectiveness Network (DSEN) “to acknowledge the limitation of pre-approval clinical trials” and to provide a mechanism “by which real world use of approved drugs can be analysed” (Senate of Canada 2013, 6). It is a step forward, but Canada’s postapproval monitoring of drug safety and effectiveness still has important weaknesses. For instance, the DSEN “has no authority to act on the information that it acquires through these studies or the ability to ensure that its findings are acted upon” (Senate of Canada 2013, 13). In addition, Health Canada does not make publicly available the safety and efficacy data of approved drugs currently on the market (Senate of Canada 2013, 19).
Lacking access to essential information from objective sources, physicians are often unaware that they are prescribing off-label. Indeed, the disturbing reality is that “a lot of the knowledge that physicians have about medicines has been acquired through sales representatives from pharmaceutical companies” (Senate of Canada 2014a, 10-11). Although drug manufacturers are prohibited by law from promoting off-label use of their products, pharmaceutical sales representatives do mention off-label indications to primary care physicians in 13 percent of drug-specific promotions (Senate of Canada 2014a, 11).
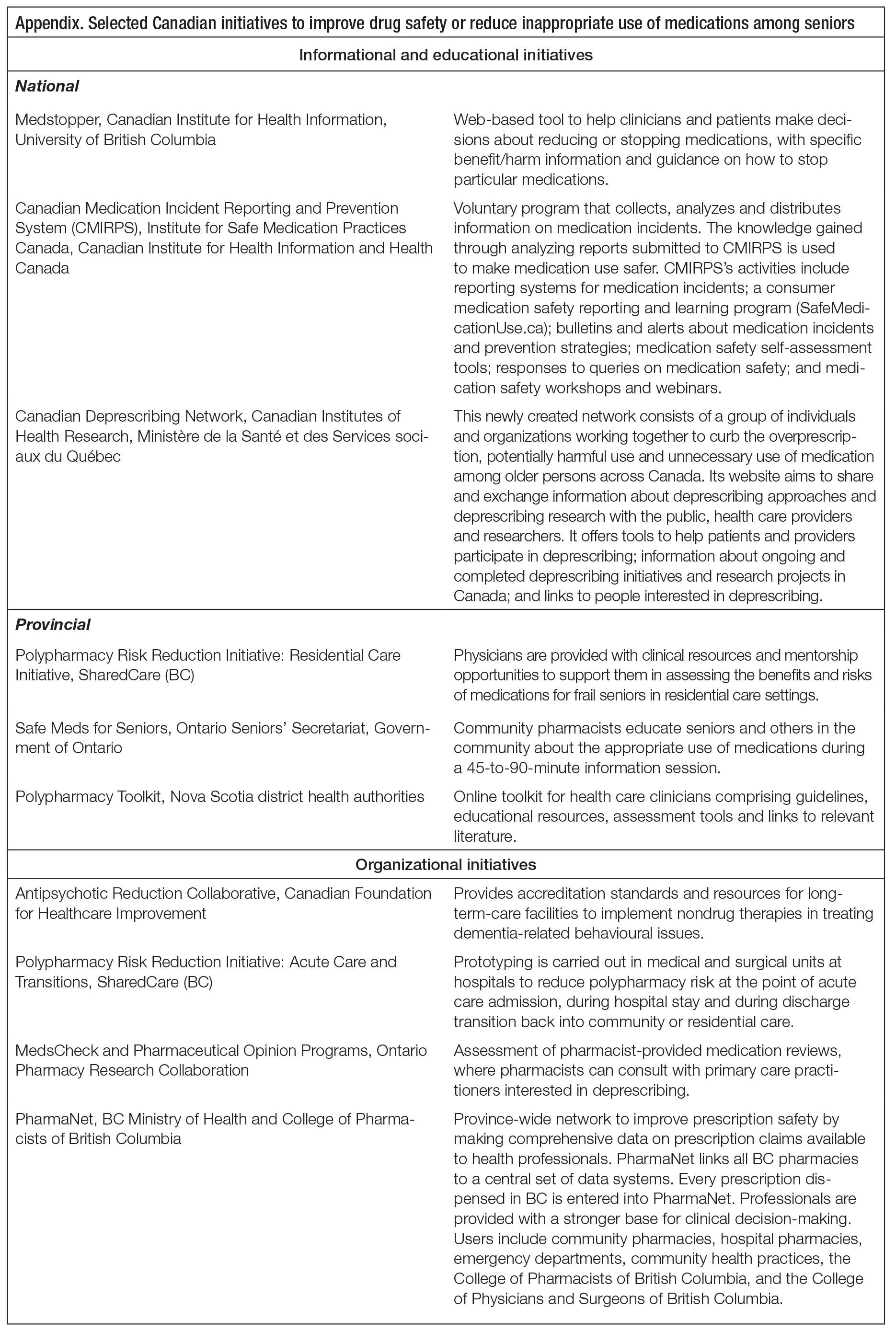
Senators Kelvin K. Ogilvie, chair of the Senate committee, and Art Eggleton, the deputy chair, openly criticized “Health Canada’s passive role in drug regulation, its lack of transparency in relaying safety information to the public; its inability to conduct adequate inspections at all phases of a drug’s life-cycle” (Ogilvie and Eggleton 2015). The committee made several recommendations that are relevant to unsafe and inappropriate prescription drug use by seniors. Before reviewing them, I present an overview of three types of initiative — informational/educational, organizational and regulatory — that could be built on to address the issue. The appendix provides additional information on these initiatives.
The most common response to the problem of drug safety among seniors in Canada has consisted of disseminating information and providing educational resources for professionals, -patients or patients’ families. Typically, professional groups such as pharmacists, doctors and nurses join efforts with advocacy groups, academics, health authorities or governments to develop joint initiatives.
One example is Medstopper. This is a Web-based tool created by a group of Canadian experts in evidence-based medicine and in prescribing for the elderly who have collaborated to help clinicians and patients make decisions on reducing or stopping medications. It provides specific benefit/harm information and guidance on stopping particular medications. It is funded by the Canadian Institute for Health Information and is administered through the University of British Columbia.
Another example is the Polypharmacy Risk Reduction Initiative in British Columbia. This is a joint effort of the Doctors of BC and the BC Ministry of Health to reduce polypharmacy risks for elderly patients. Its first phase is the Residential Care Initiative, which provides physicians across the province with clinical resources and mentorship opportunities to better assess the benefits and risks of medications for frail seniors in residential care settings.
More recently established, the Canadian Deprescribing Network is a group of individuals and organizations working together to curb overprescription and the potentially harmful and unnecessary use of medication for older people across Canada. It is the first pan-Canadian, bottom-up initiative to address this serious problem. The network’s activities focus on patient awareness, health professional outreach and policy levers, with a view to reducing inappropriate prescriptions by promoting safer alternative forms of therapy. The network provides -information and education on how to deprescribe: that is, to safely remove some drugs from a patient’s list. It aims to help doctors and pharmacists improve and better monitor prescribing practices and to help older patients communicate more effectively with health professionals.
Initiatives that seek to support or transform practices at the organizational level can play a critical role in curbing inappropriate and unsafe medication use. In a paper submitted to the National Assembly, the Quebec pharmacists’ association has argued that since today’s drug therapies are increasingly complex, we need to rethink the traditional roles of doctors and pharmacists, to move beyond simply prescribing and dispensing medications (Ordre des pharmaciens du Québec, 2011). For instance, when pharmacists are integrated into a medical care team, they can follow up on a patient’s drug therapy for certain chronic diseases and adjust the dosage for prescriptions as needed. Pharmacists can also play a proactive role, such as conducting medication reviews and informing patients as well as physicians and nurses about safer medication usage. Evidence shows that when pharmacists work closely with physicians and nurses as part of a multidisciplinary care team, a patient’s drug therapy can be significantly improved
(Makowsky et al. 2009; Spinewine, Fialova and Byrne 2012).
Organizational initiatives include those aiming to reallocate roles and responsibilities between professions as well as to develop tools to support innovation. They may entail transforming the way professionals and institutions (such as hospitals, medical clinics and nursing homes) work together and manage the prescription of drugs to the elderly. Such initiatives in Canada seem to have emerged primarily in response to scandals revealing inappropriate, dangerous antipsychotic medication use in long-term-care homes. Notable is the Antipsychotic Reduction Collaborative, a program started in 2014 by the Canadian Foundation for Healthcare Improvement (CFHI). The country-wide collaborative spans 15 jurisdictions and seeks to train nursing home practitioners to use nondrug therapies to treat behavioural issues associated with dementia. It now counts 56 participating long-term-care facilities, which are offered supports and provided with accreditation standards (CFHI 2016). The initiative is based on evidence showing that when staff are trained to take a person-centred, non-pharmacological approach to managing behaviours associated with dementia, one resident out of four could be taken off antipsychotic medication without any increase in behavioural symptoms or use of physical restraints. Some of the results are impressive. In a nursing home in Kitchener, Ontario, for instance, the rate of inappropriate antipsychotic medication use dropped from 28 percent to 17 percent within only a few months. Comparable results were observed elsewhere.
In addition to its educational component, the BC Polypharmacy Risk Reduction Initiative has an organizational component that seeks to improve prescribing patterns in acute care settings. It is currently reviewing the processes at various stages of elderly patients’ interaction with the health care system — when they are admitted to hospital, during their hospital stay, and when they are discharged and transitioning back into community or residential care — to identify ways to reduce polypharmacy risk.
PharmaNet is a system that records every prescription dispensed in British Columbia, regardless of who is paying. While it is not designed specifically to curb the problems associated with seniors’ use of prescription drugs, the PharmaNet system can help address unsafe use by providing accurate medical records to community pharmacies, hospital pharmacies, emergency departments, community health practices, the College of Pharmacists of British Columbia and the College of Physicians and Surgeons of British Columbia. (The records do not include over-the-counter drugs or natural health products.)
Through financial rules and legislation, governments have the unique capacity to redefine the general context in which unsafe or inappropriate prescribing practices for seniors are taking place. These exclusive powers also give governments important administrative and moral responsibilities. Canadians can reasonably expect public health authorities to develop regulatory regimes that ensure efficient management of primary care as well as to play a decisive role as pharmaceutical regulators in ensuring the safety of patients.
Health and community programs can be designed with built-in financial incentives or disincentives to help restrict access to certain medications for high-risk groups or, alternatively, to facilitate access to nonpharmacological treatments.
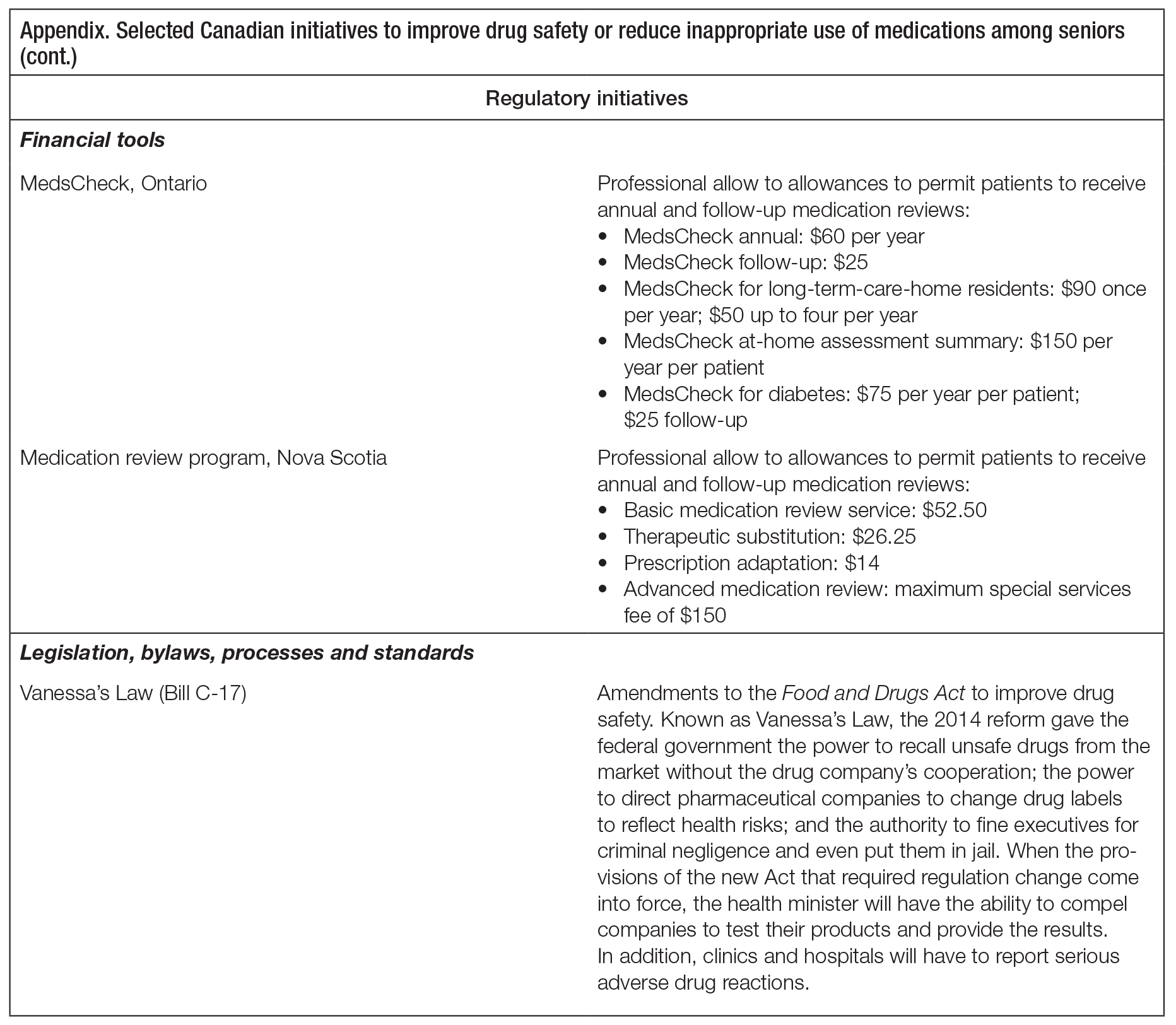
Provincial medication review programs are one common example of a financial tool used by governments to improve prescription drug safety. Under these programs, pharmacists are financially compensated for periodically assessing and documenting all the medications a patient is taking in order to optimize safe, effective and appropriate drug therapy. Medication reviews were identified as one of the top three patient safety priorities by health care leaders in every jurisdiction across Canada (Accreditation Canada et al. 2012). The Ontario MedsCheck program, created in 2007, was the first provincial program to remunerate community pharmacists for conducting medication reviews (Pammett and Jorgenson 2013). MedsCheck provides eligible patients a free 20-to-30-minute private consultation with a pharmacist.4 With the exception of Manitoba, Quebec and the territories, all jurisdictions have now adopted programs to review -patients’ medications periodically, with a professional fee schedule. But not all Canadian patients in need of a medication review may be eligible to receive one as an insured health benefit. The criteria used by each provincial program to determine a patient’s eligibility tend to focus on a risk factor (such as taking three or more medicines), and they are highly variable across the country. See the appendix for the professional allowances offered in Ontario and Nova Scotia.
As part of their regulatory role, governments can adopt or modernize legislation and bylaws, implement administrative processes, institute standards and enforce conformity to standards.
In Canada, the Food and Drugs Act regulates “any substance for which a health claim has been made,” including prescription drugs. Bill C-17, which received royal assent in late 2014, is considered the most significant reform to drug safety legislation in 50 years. Also known as Vanessa’s Law — it was adopted after a 15-year-old girl died in 2000 from the effects of a prescribed drug — it is enabling legislation that gives the federal government some of the basic regulatory instruments it was lacking to ensure drug safety in the general population. Although the bill is not fully implemented yet, Health Canada now has the power to recall unsafe drugs from the market without the drug company’s cooperation (previously, Health Canada had to negotiate with a company to get a drug off the market); the power to direct pharmaceutical companies to change drug labels to reflect health risks; and the authority to fine executives for criminal negligence and even put them in jail. When the regulations needed to implement the Bill are in place, the health minister will also be able to compel companies to test their products and provide the results.
Directly relevant to medication safety and problematic polypharmacy for seniors is the power Health Canada will have to order studies of drug safety and effectiveness specifically for the elderly (Senate of Canada 2015, 14; Health Canada 2015; Ivison 2014). In addition, clinics and hospitals will be under obligation to report serious adverse drug reactions. While this requirement looks promising, the prospects for mandatory reporting as a mechanism to enhance drug safety appear limited. One problem is that the obligation falls on clinics and hospitals, but there is still no requirement for individual health care providers to document serious adverse drug reactions. Only a fraction of ADRs are identifiable -within the existing reporting systems, and these systems are poorly adapted for use in clinical practice (Hohl, Lexchin and Balka 2015).
It is clear that much more can be done. When it comes to Canadian seniors’ health care, too many prescribing practices are based on little or no evidence and are inappropriate and even dangerous. Government reports and academic journals have addressed some of the risks and implications, but only recently have they come to the attention of the public.
The risks to seniors of polypharmacy and adverse drug reactions are of particular concern given Canada’s aging population. By 2036, Canadians aged 65 and older will account for 25 percent of the population, as compared with 16 percent today (Handren 2015, 6). But in fact everyone is at risk of being prescribed inappropriate, unsafe medication. In a recent survey of persons aged 6 to 79 living in the community, 41 percent reported having taken at least one prescription medication in the two days preceding the interview (Rotermann et al. 2014, 1). So by seeking to improve the safety of medication for seniors, policy-makers could also help improve everyone’s welfare.
Clearly physicians, before prescribing any medicine or drug mix to seniors, should be fully aware of the risks involved for these patients; they should be able to recognize ADRs in patients and should report ADRs to health authorities. Achieving these minimal goals, however, could be surprisingly difficult in Canada’s current system, where the basic tools required are inadequate or nonexistent (Senate of Canada 2013, 22). Physicians and pharmacists need better training, more information on prescription drug use by the elderly, access to patients’ full medical records, including their current drug prescriptions, and incentives to consult with other professionals as needed. Ideally, physicians should consider nondrug therapies first when treating elderly patients, but since many patients have no coverage for such alternatives, progress is unlikely to be made on that front.
What individuals, professionals and stakeholder groups can accomplish to improve the current situation is both valuable and of limited effectiveness overall, simply because the initiatives within their reach — such as developing clinical tools and forming professional networks — can only address narrower aspects of a much bigger problem. Recognizing the intrinsic limitations of such an approach is essential. Efforts by health professionals and organizations can be effective and successful only to the extent that the regulatory context supports them.
Canada needs a proactive, comprehensive strategy to eradicate the problems associated with the use of inappropriate, unsafe prescription medicines and polypharmacy among seniors. To be effective, this strategy will require putting in place proper administrative and legislative standards, rules and processes, as well as clear accountability mechanisms and sanctions. It cannot be implemented without the authority and regulatory power of Health Canada, provincial and territorial health departments, and regional and local health authorities across Canada.
While the work of the Senate Committee on Social Affairs, Science and Technology did not focus on older patients as such, it collected and analyzed a wealth of information on the regulation of prescription medicines in Canada, including how it impacts the elderly and other at-risk populations. The committee produced 5 reports and 79 recommendations. One of its main conclusions is that Health Canada must play a much more proactive role in regulating pharmaceuticals. The committee identified three critical areas of intervention:
Further, the Senate committee recommended that the roles and mandates of the DSEN and the Canadian Agency for Drugs and Technologies in Health5 be reinforced and expanded. These organizations should carry out additional independent research on the safety and effectiveness of off-label prescription drug use and take an active role in monitoring and assessing the safety and effectiveness of prescription drugs once Health Canada has approved them for sale (Senate of Canada 2014a, 24; Senate of Canada 2015, 10). The committee also recommended that drug manufacturers or the DSEN be required to conduct studies of new drugs in relevant subgroups of the population (Senate of Canada 2013, 29). Importantly, research findings should be shared across jurisdictions wherever possible.
Health Canada has yet to issue a public statement in response to the Senate reports, so it -remains unclear whether these recommendations will ever find their way into policy-making. The change in government since the publication of the final Senate report in 2015 might explain the delay in responding, but the new government has not given any indication so far that the issue of drug safety for seniors is a priority or even a concern. It should follow up as soon as possible on the Senate’s recommendations and mandate Health Canada to develop, make public and implement a comprehensive action plan with set goals, timelines and reporting mechanisms. It must also provide the necessary resources to get this work done.
Beyond these measures, there is certainly a need for a detailed examination of the unprecedented rise of unsafe, inappropriate medication use among seniors specifically. This problem needs to be examined not only as a clinical or financial issue but also as a multifaceted social phenomenon of growing concern. In order to build on the Senate committee’s work, the minister of health should mandate the Council of Canadian Academies to provide an evidence-based, authoritative assessment of the state of research and regulations leading to the approval of therapeutic products for the elderly in Canada and abroad and the effectiveness and safety of medicines prescribed to older people in Canada. The Council of Canadian Academies is an independent, not-for-profit organization that supports independent, science-based expert assessments, providing government decision-makers, researchers and stakeholders with high-quality information necessary to develop policy. The council is well suited to the task, having carried out an analysis of therapeutic products intended for infants, children and youth (Council of Canadian Academies 2014). A similar panel could be mandated to study current drug use among the elderly, including off-label use; examine the gaps in current knowledge; identify leading initiatives across Canada and elsewhere that are effective in reducing unsafe and inappropriate use of medications by older adults; and propose a strategy for improving medication-prescribing practices to ensure safe and effective medication use.
The importance of collecting, disseminating and analyzing data and information cannot be overstated. Together, health authorities across the country have the responsibility to ensure that professionals have access to accurate and comprehensive information on patient history and clinical decision-making tools that can confidently be relied upon to avoid medications and drug mixes that are inappropriate for older patients.6 Health Canada should take meaningful action to work cooperatively with provincial or territorial governments, regional and local health authorities, and other stakeholders to achieve these goals. Provinces should implement electronic prescribing and ensure the effective implementation of the long-awaited electronic systems for medical records, health records and records of dispensed prescription drugs (Senate of Canada 2014a, 24; Senate of Canada 2015, 10).
As part of an effective strategy, provinces and territories should update prescribing guidelines regularly and require medication reviews. Health care institutions as well as physicians should be required to set up control mechanisms to ensure adverse drug reactions in older patients are systematically identified, reported and investigated. These efforts will be fully effective, however, only if physicians and pharmacists receive adequate training and continuing education in the care of the elderly (including the risks of overmedication and adverse drug reactions in seniors). Although it would be helpful to have more doctors trained as geriatricians, the reality is that caring for seniors falls mostly to family physicians. These professionals also need access to proper clinical decision-making tools and better reporting systems for use in clinical practice. Improving prescribing practices in clinical settings may initially require implementing audit programs in each province and territory through which individual physicians would get feedback on their prescribing patterns.
Provincial and territorial pharmacare programs should also be extended to provide broader and more systematic coverage of effective nondrug therapies whenever appropriate, to treat older patients with chronic conditions. The Canadian Deprescribing Network proposes that governments use drug coverage eligibility rules as financial incentives to divert demand for potentially dangerous prescription medicines toward alternative treatments, such as specialized services for pain management, physiotherapy, nutrition or cognitive behavioural therapy. The rules could also include disincentives for certain prescribing practices for at-risk populations, such as long-acting sulfonylurea drugs or sleeping pills for seniors. In the network’s view, the crux of the problem of polypharmacy among seniors is that nonpharmacological treatment alternatives are neither accessible nor reimbursed for the majority of older adults.7
It is urgent that hospitals in this country implement a clear and systematic plan to improve prescribing practices when older patients visit the emergency department, are admitted to their institutions, or are discharged back to residential care or the community. As recommended by the Senate committee, they could emulate the practices of the BC Polypharmacy Risk Reduction Initiative in acute care settings (Senate of Canada 2013, 29). Such initiatives remain too limited in number and in scope and could be better developed.
One easily implementable recommendation would be for the federal government to give all Canadians access to the Cochrane Library of systematic reviews of primary research. Cochrane Reviews are internationally recognized as the highest standard in evidence-based health care resources.8 At present, only residents of New Brunswick and Nova Scotia have full free access to Cochrane Reviews. Acquiring a national licence would provide all Canadians with free online access to the most reliable evidence on prescription drug use.
Governments so far have relied too heavily on the voluntary efforts of professional groups and patients, while neglecting their own unique steering powers: that is, their capacity to design, adopt and use legislation and financial instruments to achieve desired outcomes. Ensuring the safety of the medications used by Canada’s older patients requires governments to streamline processes, regulate professional practices, provide appropriate incentives, and implement adequate financing rules, reporting and accountability mechanisms, and solid monitoring systems. By taking on a leadership role, Health Canada, provincial health departments, and -regional and local health authorities can do more and do it much better.
I thank the two external reviewers for their helpful insights and suggestions, David Deault-Picard and Colin Chia for research assistance, and Denise Avard for her valuable input at the beginning of the project.
Accreditation Canada, Canadian Institute for Health Information, Canadian Patient Safety Institute, and Institute for Safe Medication Practices Canada. 2012. Medication Reconciliation in Canada: Raising the Bar — Progress to Date and the Course Ahead. Ottawa: Accreditation Canada.
Allin, S., D. Rudoler, and A. Laporte. 2015. “Does Increased Medication Use among Seniors Increase Risk of Hospitalization and Emergency Department Visits?” Working paper. Toronto: Canadian Centre for Health Economics.
Bajcar, J.M., L. Wang, R. Moineddin, J.X. Nie, C.S. Tracy, and R.E. Upshur. 2010. “From Pharmaco-therapy to Pharmaco-prevention: Trends in Prescribing to Older Adults in Ontario, Canada, 1997-2006.” BMC Family Practice 11 (1): 1-6.
Bindslev, J.B.B., J. Schroll, P.C. Gøtzsche, and A. Lundh. 2013. “Underreporting of Conflicts of Interest in Clinical Practice Guidelines: Cross Sectional Study.” BMC Medical Ethics 14 (1): 1.
British Columbia. 2015. Office of the Seniors Advocate. Placement, Drugs and Therapy…We Can Do Better. Report 3. British Columbia, Victoria: Office of the Seniors Advocate British Columbia.
Bruser, D. 2014. “Use of Antipsychotics Soaring at Ontario Nursing Homes.” Toronto Star, April 15. Ottawa: Canadian Foundation for Healthcare Improvement. Accessed October 2, 2016. https://www.thestar.com/news/canada/2014/04/15/use_of_antipsychotics_soaring_at_ontario_nursing_homes.html.
Canada. 2016. “An Inclusive and Fair Canada. ” In Budget 2016. Ottawa: Government of Canada. Accessed October 3, 2016. https://www.budget.gc.ca/2016/docs/plan/ch5-en.html
Canadian Foundation for Healthcare Improvement. 2016. Reducing Antipsychotic Medication Use Collaborative. Ottawa: Canadian Foundation for Healthcare Improvement. Accessed April 29, 2016. https://www.cfhi-fcass.ca/WhatWeDo/reducing-antipsychotic-medication-use-collaborative
Canadian Institute for Health Information (CIHI). 2010. Drug Use among Seniors on Public Drug Programs in Canada, 2002 to 2008. Ottawa: CIHI.
———. 2011. Health Care in Canada, 2011: A Focus on Seniors and Aging. Ottawa: CIHI.
———. 2013. Adverse Drug Reaction-Related Hospitalizations among Seniors, 2006 to 2011. Ottawa: CIHI.
———. 2014. Drug Use among Seniors on Public Drug Programs in Canada, 2012. Ottawa: CIHI.
———. 2016. Use of Antipsychotics among Seniors Living in Long-Term Care Facilities, 2014. Ottawa: CIHI.
Chief Public Health Officer. 2010. Annual Report on the State of Public Health in Canada, 2010: Growing Older — Adding Life to Years. Ottawa: Public Health Agency of Canada.
CIHI (see Canadian Institute for Health Information).
College of Physicians and Surgeons of Ontario. 2016. Prescribing Drugs. Policy Statement 3-16. Toronto: College of Physicians and Surgeons of Ontario.
Council of Canadian Academies. 2014. Improving Medicines for Children in Canada: Executive Summary. Ottawa: Council of Canadian Academies.
Davison, C., and M. Perron. 2013. First Do No Harm: Responding to Canada’s Prescription Drug Crisis. Ottawa: Canadian Centre on Substance Abuse.
Duerden, M., T. Avery, and R. Payne. 2013. Polypharmacy and Medicines Optimisation: Making It Safe and Sound. London, UK: King’s Fund.
Eguale T., D.L. Buckeridge, N.E. Winslade, A. Benedetti, J.A. Hanley, and R. Tamblyn. 2012. “Drug, Patient, and Physician Characteristics Associated With Off-Label Prescribing in Primary Care.” Archives of Internal Medicine, 172 (10): 781-8.
Frank, C. 2014. “Deprescribing: A New Word to Guide Medication Review.” Canadian Medical Association Journal 186 (6): 407-8.
Gamble, J.M., J.J. Hall, T.J. Marrie, C.A. Sadowski, S.R. Majumdar, and D.T. Eurich. 2014. “Medication Transitions and Polypharmacy in Older Adults Following Acute Care.” Therapeutics and Clinical Risk Management 10: 189-96.
Handren, L. 2015. Unfilled Prescriptions: The Drug Coverage Gap in Canada’s Health Care System. Toronto: Mowat Centre.
Health Canada. 2015. “Protecting Canadians from Unsafe Drugs Act (Vanessa’s Law): Amendments to the Food and Drugs Act (Bill C-17).” Ottawa: Health Canada. Accessed June 17, 2016. https://www.hc-sc.gc.ca/dhp-mps/legislation/unsafedrugs-droguesdangereuses-eng.php.
Hohl, C., J.R. Lexchin, and E. Balka. 2015. “Can Reporting of Adverse Drug Reactions Create Safer Systems while Improving Health Data?” Canadian Medical Association Journal 187 (11): 789-90.
Hohl, C.M., P.J. Zed, J.R. Brubacher, R.B. Abu-Laban, P.S. Loewen, and R.A. Purssell. 2010. “Do Emergency Physicians Attribute Drug-Related Emergency Department Visits to Medication-Related Problems?” Annals of Emergency Medicine 55 (6): 493-502.
Ivison, J. 2014. “MP’s 14 Year Mission to Make Prescription Drug Use Safer Nearly over with Law Named after His Late Daughter.” National Post, October 7.
Kwan, D., and B. Farrell. 2014. “Polypharmacy: Optimizing Medication Use in Elderly Patients.” Canadian Geriatrics Society Journal of CME 4 (1): 21-7.
Lexchin, J. 2013. “Living Better through Chemistry: Dementia, Long-Term Care, and Antipsychotic Medication Use.” In Troubling Care: Critical Perspectives on Research and Practices, edited by P. Armstrong and S. Braedley. Toronto: Canadian Scholars’ Press, 117-27.
Makowsky, M.J., T.J. Schindel, M. Rosenthal, K. Campbell, R.T. Tsuyuki, and H.M. Madill. 2009. “Collaboration between Pharmacists, Physicians and Nurse Practitioners: A Qualitative Investigation of Working Relationships in the Inpatient Medical Setting.” Journal of Interprofessional Care 23 (2): 169-84.
McPherson, M., H. Ji, J. Hunt, R. Ranger, and C. Gula. 2012. “Medication Use among Canadian Seniors.” Healthcare Quarterly 15 (4): 15-18.
Millar, W. 1998. “Multiple Medication Use among Seniors.” Health Reports 9 (4): 11-17.
Morgan, S.G., J. Hunt, J. Rioux, J. Proulx, D. Weymann, and C. Tannenbaum. 2016. “Frequency and Cost of Potentially Inappropriate Prescribing for Older Adults: A Cross-Sectional Study.” CMAJ Open 4 (2): E346-351.
Neuman, J., D. Korenstein, J.S. Ross, and S. Keyhani. 2011. “Prevalence of Financial Conflicts of Interest among Panel Members Producing Clinical Practice Guidelines in Canada and United States: Cross Sectional Study.” BMJ 343: d5621.
Norris, S.L., H.K. Holmer, L.A. Ogden, B.U. Burda, and R. Fu. 2013. “Conflicts of Interest among Authors of Clinical Practice Guidelines for Glycemic Control in Type 2 Diabetes Mellitus.” PLOS One 8 (10): e75284.
Ogilvie, K., and A. Eggleton. 2015. “Prescription Drug Regulation Needs Transparency and Openness.” Toronto Star, March 11.
Ordre des pharmaciens du Québec. 2011. Mémoire de l’Ordre des pharmaciens du Québec sur le projet de loi 41 modifiant la Loi sur la pharmacie. Montreal: Ordre des pharmaciens du Québec.
Page, A.T., C.D. Etherton-Beer, R.M. Clifford, S. Burrows, M. Eames, and K. Potter. 2016. “Deprescribing in Frail Older People — Do Doctors and Pharmacists Agree?” Research in Social and Administrative Pharmacy 12 (3): 438-49.
Pammett, R., and D. Jorgenson. 2013. “Eligibility Requirements for Community Pharmacy Medication Review Services in Canada.” Canadian Pharmacists Journal 147 (1): 20-4.
Patterson, S.M., C.A. Cadogan, N. Kerse, C.R. Cardwell, M.C. Bradley, C. Ryan, and C. Hughes. 2014. “Interventions to Improve the Appropriate Use of Polypharmacy for Older People.” Cochrane Database of Systematic Reviews 10.
Ramage-Morin, P.L. 2009. “Medication Use among Senior Canadians.” Health Reports 20 (1): 37-44.
Reason, B., M. Terner, A.M. McKeag, B. Tipper, and G. Webster. 2012. “The Impact of Polypharmacy on the Health of Canadian Seniors.” Family Practice 29 (4): 427-32.
Rotermann, M., C. Sanmartin, D. Hennessy, and M. Arthur. 2014. “Prescription Medication Use by Canadians Aged 6 to 79.” Health Reports 25 (6): 3-9.
Senate of Canada. 2013. Standing Senate Committee on Social Affairs, Science and Technology. Prescription Pharmaceuticals in Canada: Post-Approval Monitoring of Safety and Effectiveness. Ottawa: Senate of Canada.
———. 2014a. Standing Senate Committee on Social Affairs, Science and Technology. Prescription Pharmaceuticals in Canada: Off-Label Use. Ottawa: Senate of Canada.
———. 2014b. Standing Senate Committee on Social Affairs, Science and Technology. Prescription Pharmaceuticals in Canada: Unintended Consequences. Ottawa: Senate of Canada.
———. 2015. Standing Senate Committee on Social Affairs, Science and Technology. Prescription Pharmaceuticals in Canada: Final Report. Ottawa: Senate of Canada.
Seniors at Risk. 2012. “It’s ‘Snowing’ in BC — Staff Term for Drugging of Nursing Home Residents,” August 23. N.p.: Seniors at Risk. Accessed April 29, 2016. https://www.seniorsatrisk.org/?s=snowing.
Spinewine, A., D. Fialova, S. Byrne. 2012. “The Role of the Pharmacist in Optimizing Pharmacotherapy in Older People.” Drugs & Aging 29 (6): 495-510.
Spurling, G.K., P.R. Mansfield, B.D. Montgomery, J. Lexchin, J. Doust, N. Othman, and A.I. Vitry. 2010. “Information from Pharmaceutical Companies and the Quality, Quantity, and Cost of Physicians’ Prescribing: A Systematic Review.” PLOS Medicine 7 (10): e1000352.
Steinman, M.A., L.A. Bero, M.M. Chren, and C.S. Landefeld. 2006. “Narrative Review: The Promotion of Gabapentin: An Analysis of Internal Industry Documents.” Annals of Internal Medicine 145 (4): 284-93.
Stueck, W. 2012. “Half of Elderly in Residential Care on Anti-psychotic Drugs.” Globe and Mail, January 15. Accessed October 3, 2016. https://www.theglobeandmail.com/life/health-and-fitness/half-of-elderly-in-residential-care-on-anti-psychotic-drugs/article1358558/.
Van Zee, A. 2009. “The Promotion and Marketing of Oxycontin: Commercial Triumph, Public Health Tragedy.” American Journal of Public Health 99 (2): 221-7.
Walkom, T. 2016. “Government Still Lets Nursing Homes Improperly Drug Seniors.” Toronto Star, May 18. Accessed October 3, 2016. https://www.thestar.com/opinion/commentary/2016/05/18/government-still-lets-nursing-homes-improperly-drug-seniors-walkom.html.
Zou, D., and C. Tannenbaum. 2014. “Educational Needs, Practice Patterns and Quality Indicators to Improve Geriatric Pharmacy Care.” Canadian Pharmacists Journal 147 (2): 110-17.
This study was published as part of the Faces of Aging research program under the direction of France St-Hilaire. Copy editing was by Barbara Czarnecki, proofreading was by Mary Williams, editorial coordination was by Francesca Worrall, production was by Chantal Létourneau and art direction was by Schumacher Design.
Nicole F. Bernier is a researcher and writer on Canadian health and social policy. She worked from 2011 to 2016 as research director of the Faces of Aging research program at the Institute for Research on Public Policy (IRPP).
To cite this document:
Bernier, Nicole F. 2017. Improving Prescription Drug Safety for Canadian Seniors. IRPP Study 61. Montreal: Institute for Research on Public Policy.
Montreal – Canada needs a national strategy to address inappropriate prescribing practices that lead to the unsafe use of medications by seniors, says the author of a new study from the Institute for Research on Public Policy.
Seniors are the heaviest users of prescription medicines in Canada. On average, two-thirds take 5 or more prescriptions drugs over the course of a year and one-quarter take 10 or more, says Nicole Bernier. “It is estimated that as much as half of the medications given to seniors are taken incorrectly or are overprescribed, increasing the likelihood of adverse drug reactions and interactions.”
Bernier observes that governments have relied heavily on the voluntary efforts of professional groups and patients to address the issue, when they could use legislation and financial instruments to much greater effect.
She calls for a comprehensive strategy and a more proactive role for Health Canada. Building on the 2015 recommendations of the Senate Committee on Social Affairs, Science and Technology, such a strategy would entail revising the drug approval process, monitoring newly marketed drugs prescribed to seniors, improving reporting on adverse drug reactions, and encouraging independent research into off-label prescription drug use.
Additionally, provinces and territories would be required to update their prescribing guidelines regularly, require medication reviews, and provide coverage for effective nondrug therapies. Health authorities would need to ensure that professionals have access to clinical decision-making tools, as well as accurate and comprehensive information on patients’ medical histories, in order to improve prescribing practices overall.
“When it comes to seniors’ health, prescribing practices are too often based on little or no evidence, and as a result they can be inappropriate and even dangerous. Much more can and should be done to address this serious health issue for our aging population,” Bernier concludes.
Improving Prescription Drug Safety for Canadian Seniors, by Nicole F. Bernier, can be downloaded from the Institute’s website (irpp.org).
-30-
The Institute for Research on Public Policy is an independent, national, bilingual, not-for-profit organization based in Montreal. To receive updates from the IRPP, please subscribe to our e-mail list.
Media contact: Shirley Cardenas tel. 514-594-6877 scardenas@nullirpp.org
Four years ago, at age 84, my dad survived a severe stroke. The downside is that during his hospital stay this otherwise fit person was put on a drug regimen and has been taking nine prescription drugs a day ever since.
My dad’s experience with multiple drugs is not uncommon for his age group. Seniors age 65 and over are the heaviest users of prescription drugs in the country. They take, on average, 7.4 prescription drugs.
Experts have pointed to increased drug utilization as a driver of health care spending in Canada for some years, but safety issues are increasingly salient. Seniors are five times more likely than younger Canadians to be hospitalized as a result of an adverse drug reaction (ADR). In 2011, over 27,000 Canadian seniors — that is, one in 200 — had an ADR-related hospitalization.
Seniors face a higher risk of adverse drug reactions, in part because of physiological changes as we age that alter the way our bodies respond to medication (pharmacokinetics) and process them (pharmacomdynamics). For instance, our kidneys and liver tend to lose functional ability and become less efficient in flushing out drugs.
Many drugs prescribed to seniors have either not been adequately studied for this age group or have not been formally approved for the conditions they are being prescribed to treat. They are sometimes prescribed without any evidence they are safe and effective for them, and in some cases, even when they are known to present a possible risk (antipsychotics prescribed to older patients with dementia, for example).
It is estimated that as much as half of the medications given to seniors are taken incorrectly or are prescribed in an excessive manner.
Clinical trials often exclude not only older people, but also people of all ages who take a combination of medications. On average, two-thirds of seniors take five or more prescriptions drugs over the course of a year — one-quarter take 10 or more. The prevalence of polypharmacy (multiple medications) has been rising from 54.7 percent of seniors using five prescription drugs or more in 2000 to 66.1 percent in 2014.
The dangers of polypharmacy for seniors are seen in doctors’ offices and hospitals. The more medications they consume, the more likely seniors are to require urgent medical attention or go to emergency departments. A study found that 12 percent of Canadian seniors taking five or more medications have experienced an adverse reaction requiring medical attention.
Clearly, we need a solution.
In a new Institute for Research on Public Policy Study (IRPP) study, I have documented several collaborative initiatives undertaken by professionals, advocacy groups and health authorities, which seek to provide information and educational resources, reallocate roles and responsibilities and promote innovation. While they are all valuable, their overall effectiveness is limited, because they address only narrow aspects of a much bigger problem.
Improving drug safety among seniors requires systemic change.
Governments could use legislation and financial instruments to much greater effect to steer the country’s efforts in the right direction. Required is a comprehensive national strategy which involves leadership and engagement from Health Canada, provincial and territorial health ministries and local health authorities.
Building on the 2015 recommendations of the Senate Committee on Social Affairs, Science and Technology, such a strategy would entail revising the drug approval process, monitoring newly marketed drugs prescribed to seniors, improving reporting on adverse drug reactions and encouraging independent research into off-label prescription drug use.
Provincial and territorial pharmacare programs should also be extended to provide broader and more systematic coverage of effective nondrug therapies whenever appropriate, to treat older patients with chronic conditions.
Provinces and territories would be required to update their prescribing guidelines regularly and require medication reviews. Health authorities would need to ensure that professionals have access to clinical decision-making tools, as well as accurate and comprehensive information on patients’ medical histories, in order to improve prescribing practices overall.
Clearly, much more can and should be done by governments to address this serious health issue for our aging population.
Nicole F. Bernier is a researcher and writer on Canadian health and social policy and expert adviser with EvidenceNetwork.ca. She worked from 2011 to 2016 as research director at the Institute for Research on Public Policy and is the author of an IRPP Study entitled, Improving Prescription Drug Safety for Canadian Seniors.
Seniors are the heaviest users of prescriptions medicines in Canada. Yet it is estimated that as much as half of the medications given to seniors are taken incorrectly or overprescribed, increasing the likelihood of adverse drug reactions and interactions. Moreover, many drugs prescribed to seniors either have not been adequately studied for this age group or have not been formally approved for the conditions they are being prescribed to treat. What are the principal causes and what is the extent of the problem? What more can be done to address this serious health issue for our aging population? Panelists Nicole F. Bernier, former director of the IRPP’s Faces of Aging program, Isobel Mackenzie, BC Seniors Advocate, and Dr. Joel Lexchin, Professor Emeritus at York University discussed these questions and more.




