Securing Natural Capital and Ecological Goods and Services for Canada
Policy brief
Nancy Olewiler
Evans, Hertzman and Morgan’s proposals to improve health outcomes in Canada address two distinct determinants of good health: actions that influence whether people become ill or injured and those that support responses to those illnesses or injuries. Their first proposal, a universal early childhood development (ECD) program, draws upon a large body of evidence that shows the main reason that some people are healthy and others not is rooted in the conditions in which they live and work. Their second proposal calls for a major reorientation of the funding and regulation of pharmaceuticals in Canada that could dramatically improve their cost-effectiveness. Finally, they propose a standardized electronic medical record system to improve clinical decision-making.
Although she supported the three policy proposals, commentator Raisa Deber felt that they were detached from current political reality and also pointed out that difficult federal-provincial relations issues were addressed only in passing. Commentator Dennis Raphael argued that reducing Canada’s high poverty rate is even more important than the chosen policy suite.
Canada, like all high-income countries, spends far more on its health care system than on upstream efforts to improve health status at the population level.
The authors observe that Canada, like all high-income countries, spends far more on its health care system than on upstream efforts to improve health status at the population level. Canadians are already among the healthiest people in the world. However, the persistence of large inequalities in health across socioeconomic groups indicates that there is still considerable room for improvement. The authors report that more than 25 percent of Canadians reach adulthood without the competencies they need to cope in the modern economy.
For virtually every indicator, those lower down the socioeconomic scale have, on average, poorer health. This social gradient is universally observed and widely studied. Propensity to unhealthy behaviours does not arise randomly in a population; it emerges from a particular social context. “The experiences of early childhood become ” embedded’ in the form of patterns of response to later stresses, not only as healthy or unhealthy behaviour, but also as learned biological responses through the endocrine and cardiovascular systems that may support or damage health.”
Even though it is not the primary determinant of health outcomes, the health care system has been the primary focus of public debate in Canada, with regard to both funding and service delivery. The share of health in provincial government spending has increased dramatically, leading many to claim that rising health care expenditures are “crowding out” other public programs. While the authors take issue with the notion that public health care expenditures are unsustainable, the question remains whether the system could be managed more efficiently, freeing up resources for programs more likely to improve the health status of the population in the long run.
Prevention: Redress the social gradient in health
There are significant differences across countries in the steepness of the health gradient, and these differences in average health are observed at the bottom of the income scale, not the top. Scandinavian countries, for example, have relatively flat gradients, continental Europe’s is steeper, and that of the United States is markedly steeper again; Canada’s lies between those of Europe and the US. However, as the authors remark, the fact that social gradients differ shows that they can be modified. The adult gradients in health are less pronounced among children or adolescents: a good or bad start leads to a life trajectory in which good or poor outcomes at each stage reinforce the probability of success or failure at the next. Furthermore, as Raphael observed, poor health outcomes are disproportionately concentrated among low-income households. Thus the most effective policies for improving health outcomes in Canada are those that reduce the incidence and health-related consequences of poverty.
Improve the cost-effectiveness of the health care system
Irrespective of the debate over the sustainability of the public health care system, there are many opportunities to increase “value for money” in the current system that need to be exploited. In addition to improving health outcomes, this would free up resources to be invested in other activities that would redress the social gradient in health outcomes.
Hospitals and doctors absorb half of all health care spending and two-thirds of public spending, although this share has been essentially stable as a share of GDP. But there is growing evidence of wide variations in clinical practice and a steady growth in increasingly expensive diagnostic and therapeutic interventions, both without evidence of improved outcomes.
The fastest-growing component of health costs is out-of-hospital prescription drugs. Between 1975 and 2006, expenditures on prescription drugs as a share of total health costs rose from 6.3 percent to 14.3 percent. According to the authors, this uncontrolled cost escalation is the result of Canada’s fragmented funding system for pharmaceuticals.
Implement a universal, comprehensive early childhood development (ECD) program
To prevent poor health outcomes and to address the social determinants of health, the authors propose a comprehensive early childhood development program. Their proposal would require the federal government to negotiate with the provinces to reinstate the Early Learning and Child Care transfer program. The aim of negotiations on resource transfers would be agreements on the standards against which funding for a full network of centres would follow. ECD would provide but go well beyond universal daycare, to address the full range of factors shown to promote optimal child development, such as parental leave and newborn screening and follow-up. The authors estimate the cost of such a program to be $20 billion to $25 billion annually, which would be similar (as a percentage of GDP) to what is spent in Scandinavia.
The following proposals to improve the cost-efficiency of the health care system would help the government meet this ECD funding target.
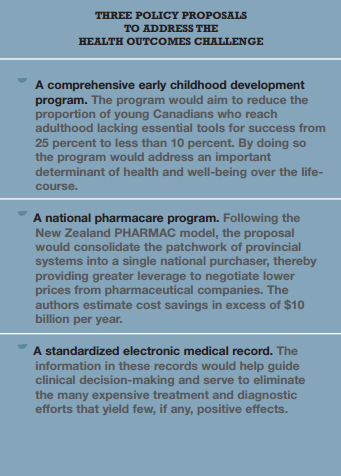
Implement a national pharmacare program
The authors propose to retain comprehensive pharmacare for seniors and social assistance recipients and offer full first-dollar coverage for drugs to treat specific health conditions for the whole population.The program, based on the New Zealand model, would be strictly managed by a national, publicly accountable agency and cover only evidence-based and cost-effective drugs.The costs would be borne evenly by federal and provincial governments with patient co-payments (if desired) limited to the pharmacist’s dispensing fee. The authors provide evidence that the escalation of drug costs can be contained by a single-buyer regime, but Deber pointed out that it may be difficult to reconcile the competing goals of guaranteed access and low cost.
Develop a standardized electronic medical record (EMR)
A more explicitly evidence-based approach to clinical decision-making within the public system could considerably advance the health and well-being of Canadians: a clinical information system “would provide the information base from which medical necessity, or perhaps better evidence of health outcome, could drive clinical practice.” Moreover, the EMR has the potential for system-wide rapid learning through the online assembly and assessment of a vast array of clinical experience, and consequent significant improvement in health outcomes.There is some evidence that this has been effective elsewhere, although Deber pointed out that the EMR’s effectiveness may be limited if institutional or systemic barriers hamper its use.
Irrespective of the debate over the sustainability of the public health care system, there are many opportunities to increase “value for money” in the current system that need to be exploited.
Socio-economic factors are the most powerful determinants of health status at the population level and for this reason the authors choose a comprehensive ECD program as their main proposal. It is critical that a national ECD program be universal and adequately funded. Targeting, they write, “not only tends to ghettoize the program participants as children of socially inadequate families; it also abandons significant numbers of children with problems whose families are not poor.” However, the health care system should not be overlooked: “The opportunity costs of inefficiency are correspondingly high; a 10 percent saving in health care could fund over half the cost of a very broadly based national childhood development program.” Finally, further efficiencies stand to be gained through a comprehensive clinical information system.