

Au Canada, l’assurance médicaments est une mosaïque de régimes publics provinciaux, territoriaux et fédéraux, d’assurances privées et de paiements directs. Des millions de Canadiens n’ont pas les moyens d’acheter les médicaments qui leur ont été prescrits. Mais nous avons l’occasion de changer cette situation. Le gouvernement libéral fédéral a signé un accord de soutien et de confiance avec le Nouveau Parti démocratique qui comprend l’engagement d’introduire un régime national d’assurance médicaments. Il existe plusieurs modèles que le gouvernement pourrait utiliser pour mettre en œuvre un tel régime. Le présent document préconise une approche par étapes, prudente sur le plan financier, en commençant par un programme fédéral de réassurance pour les médicaments coûteux destinés au traitement des maladies rares, qui jetterait les bases d’un régime d’assurance médicaments complet et universel.
L’assurance médicaments a été inscrite à de nombreuses reprises à l’ordre du jour des politiques au Canada. Pratiquement toutes les commissions sur la santé depuis les années 1960 ont demandé une certaine forme de couverture standard pour une liste complète de médicaments. Pourtant, la couverture des médicaments au Canada reste une mosaïque de régimes publics provinciaux, territoriaux et fédéraux, d’assurances privées et de dépenses à même la poche des ménages. Il en résulte des niveaux de couverture différents, tant à l’intérieur d’une même juridiction qu’entre les différentes juridictions. Des millions de Canadiens n’ont pas les moyens d’acheter les médicaments qui leur ont été prescrits par un médecin.
Il existe une fenêtre d’opportunité pour améliorer cette situation. Le gouvernement fédéral a pris des mesures initiales en faveur d’un régime national d’assurance médicaments dans son budget 2019. Il a annoncé la création de l’Agence canadienne des médicaments, qui serait notamment chargée de dresser une liste nationale des médicaments à couvrir, d’évaluer leur efficacité et de négocier leurs prix avec les compagnies pharmaceutiques. Le gouvernement a également déclaré qu’il créerait une stratégie nationale sur les médicaments à coût élevé pour les maladies rares. Il a alloué plus d’un milliard de dollars à l’élaboration de cette stratégie et à la création de l’agence. L’élan s’est renforcé en mars 2022 lorsque les libéraux au pouvoir ont signé une entente de soutien et de confiance avec le Nouveau Parti démocratique qui comprenait l’engagement d’adopter une loi sur le régime d’assurance médicaments du Canada avant la fin de l’année 2023. Cela ne s’est pas produit, mais les partis ont récemment convenu d’un nouveau délai, fixé au 1er mars 2024.
Un facteur clé dans le débat sur le régime national d’assurance médicaments est le coût public, que le Bureau parlementaire du budget a estimé à 11,2 milliards de dollars en 2024-2025 si la liste nationale des médicaments était la même que celle utilisée par le régime provincial du Québec. Il existe cependant de nombreux modèles que les décideurs politiques pourraient suivre pour passer à un régime national. Il s’agit notamment de limiter la couverture à un petit nombre de médicaments essentiels ou d’établir un plan qui se concentrerait sur la couverture des médicaments coûteux par rapport aux revenus des ménages.
Un plan efficace doit rendre les médicaments sur ordonnance plus abordables et plus accessibles pour tous les Canadiens, en supprimant les obstacles liés au coût et en réduisant les inégalités entre les sexes, entre les niveaux de revenus, entre les provinces, entre ceux qui ont une assurance privée et ceux qui n’en ont pas, ainsi qu’entre les communautés des Premières Nations. Il doit améliorer la manière dont les médicaments sont prescrits et utilisés. Enfin, il doit être pratique. Il devrait d’abord cibler les domaines où les besoins sont les plus importants, minimiser les perturbations de la couverture existante et de l’utilisation des médicaments, s’inscrire dans le cadre des budgets disponibles et être conçu pour couvrir, à terme, tous les Canadiens. Compte tenu de ces éléments et de la nécessité d’adopter une approche financièrement viable en matière d’assurance médicaments nationale, nous proposons et recommandons un régime de réassurance géré par le gouvernement fédéral qui commencerait par les médicaments coûteux.
Nous recommandons que le plan de réassurance comporte les caractéristiques suivantes :
Cette proposition présente de nombreux avantages, au-delà de l’amélioration de l’accès aux médicaments, du renforcement de l’équité du système et de l’amélioration de la manière dont les médicaments sont prescrits et utilisés au Canada. Son introduction pourrait être relativement peu coûteuse. Les dépenses futures des gouvernements seraient adaptables et prévisibles. Il fonctionnerait bien avec les régimes de couverture existants dans les provinces et les territoires. Un régime fédéral de réassurance pourrait s’appuyer sur la coopération existante entre les gouvernements fédéral, provinciaux et territoriaux pour évaluer les nouveaux médicaments et négocier les prix. Enfin, il permettrait au gouvernement fédéral de s’asseoir à la table des négociations, de préciser sa contribution financière et de créer une voie viable vers une couverture universelle plus complète et mieux coordonnée.
Cela fait plus d’un demi-siècle que les responsables politiques canadiens parlent d’un régime national d’assurance médicaments. Nous avons l’occasion de faire un pas décisif vers cet objectif. Ne la gâchons pas.
Pharmacare has risen on the policy agenda many times in Canada. Virtually every commission on health since the 1960s has called for some form of national pharmacare, meaning a plan that includes standard coverage across Canada for a comprehensive list of medicines. They included the Royal Commission on Health Services (1964), also known as the Hall Commission; the National Forum on Health (1997); the Commission on the Future of Health Care in Canada (2002), also known as the Romanow commission; the Study on the State of the Health Care System in Canada (2003), also known as the Kirby commission; and, most recently, the Advisory Council on the Implementation of National Pharmacare (2019). Despite these repeated calls, drug coverage in Canada remains a patchwork of different provincial, territorial and federal public plans, private drug insurance and out-of-pocket payments by households (Daw & Morgan, 2012). This has resulted in different levels of coverage, both within and across jurisdictions. Millions of Canadians cannot afford the drugs they have been prescribed by a physician (Holbrook et al., 2021).
The federal government announced three pharmacare initiatives in its 2019 budget: the creation of the Canadian Drug Agency to assess the effectiveness of new prescription drugs and negotiate prices on behalf of Canadians, the development of a national list of covered drugs (a formulary) and the creation of a national strategy for high-cost drugs for rare diseases. Health Canada received $35 million to spend over four years on the Canadian Drug Agency and the national formulary. The government committed up to $1 billion in funding over two years, starting in 2022, and up to $500 million a year afterwards on the strategy for high-cost drugs for rare diseases (Government of Canada, 2019). It said these steps toward a national pharmacare program would increase affordability and access.
Movement on pharmacare accelerated in March 2022 when the Liberals and the New Democratic Party struck a deal they called Delivering for Canadians Now, a Supply and Confidence Agreement. In it they agreed to continue “progress towards a universal national pharmacare program by passing a Canada Pharmacare Act by the end of 2023” (Liberal Party of Canada and the New Democratic Party, 2022). The details of the program have not been stated publicly, aside from having the Canadian Drug Agency develop a national formulary and a bulk purchasing plan. The parties were still negotiating when the 2023 deadline passed without the introduction of new legislation. Recently, a new deadline of March 1, 2024, was agreed upon.
All prior windows of opportunity for pharmacare reform closed with limited progress toward a national approach with a defined role for the federal government. However, a number of bodies and initiatives have emerged to fill some of this void. For example, public drug plans now do a centralized assessment of new brand medicines through Canada’s Drug and Health Technology Agency, an independent, not-for-profit body set up by the federal, provincial and territorial governments. The drug plans collectively negotiate drug prices through the pan-Canadian Pharmaceutical Alliance, an independent organization whose members include the federal, provincial and territorial governments. These initiatives have led to significant convergence in the formularies across the public plans but have not had a major impact on how the different plans are designed (Patented Medicine Prices Review Board, 2017). As a result, there is still significant variation across the country in who is covered by public plans and under what terms. Improving coverage and co-ordination remains a significant imperative, and a place where the federal government has a potential role to play.
In March 2023, the federal government announced further specifics on how the funding for expensive drugs for rare diseases would be used (Health Canada, 2023). A significant portion of the funding allocated over a three-year period, $1.4 billion, was earmarked for bilateral agreements with the provinces and territories to improve access to new and emerging drugs for Canadians with rare diseases. The agreements will target a specific set of new and emerging drugs that will be covered across the country. The list of drugs and the nature of the cost sharing required of the provinces, territories and patients has not yet been disclosed. The 2023 federal budget contained no additional financial commitments for drug coverage (Government of Canada, 2023).
One impediment to change is the potential cost to the public of a national pharmacare plan. The Office of the Parliamentary Budget Officer (PBO), which provides economic and financial analysis to Parliament, estimated in 2023 that national pharmacare would save money at a societal level, reducing drug expenditures by $1.4 billion in 2024-25 (Office of the Parliamentary Budget Officer, 2023). However, it would significantly increase public spending as the government assumed responsibility for payments currently made through private insurance or by households. The PBO estimated that public expenditures would increase by $11.2 billion in 2024-25 if the national plan was based on the Quebec drug list.
It is critical that another window of opportunity does not pass without progress toward more co-ordinated and comprehensive drug coverage in Canada. In this paper, we outline how to leverage the existing commitments for expensive drugs for rare diseases and lay the groundwork for national pharmacare in a way that is consistent with fiscal prudence, universality and public administration. Our plan focuses on the feasible first step of implementing a federal reinsurance program for high-cost medications. It builds on the funding for high-cost drugs for rare diseases that has already been committed and creates a platform for staged expansion that could eventually achieve a full and comprehensive program of consistent universal public drug coverage across Canada.
This proposal builds on the following key goals:
Policy change in this area is contentious. We address this concern by proposing the following principles for implementation:
Working from the above goals and principles, it is possible to assess the various options available to policymakers for developing a universal approach to national pharmacare. There are several potential models for transitioning to a more comprehensive program (Law et al., 2018). Recent debates have largely focused on two main options. The first would start with coverage of a small number of medicines that are deemed essential because they cover the priority needs of the population. The second is a reinsurance program that would focus on providing coverage for drugs that are expensive relative to household incomes. It is critical to assess which model would work best with the current funding for expensive drugs for rare diseases, as this dedicated funding provides a potential launchpad for a more comprehensive approach.
The Advisory Council on the Implementation of National Pharmacare advocated using the first model to transition to national pharmacare in its 2019 report. Lists of essential medicines have been used in other countries. The World Health Organization publishes a model list of essential medicines and updates it every two years (World Health Organization, 2021). The advisory council recommended that the federal government introduce coverage for a list of essential medicines and expand it over five years to include a more comprehensive list of covered drugs.
From the standpoint of feasibility, this approach is highly incompatible with the existing funding for drugs for rare diseases. While there is nothing inherent in an essential medicines list that would exclude expensive drugs, none of the current lists are composed entirely of expensive medications. The majority of the drugs on existing lists of essential medicines are lower-cost medicines, largely generics, which would not qualify for funding under the recently announced funds. In addition, the estimated cost of covering essential medicines far exceeds the funding allocated through the expensive drugs for rare diseases envelope. It may well exceed what the government is currently willing to spend. Therefore, it is difficult to see how this approach to starting national coverage would be consistent with the current funding. There are more general drawbacks that merit consideration (Health Canada, 2023). For example, the majority of Canadians already have coverage for many essential medicines. That means that new public funding would largely displace existing coverage.
The model that can feasibly adhere to the goals and principles outlined above is a reinsurance plan run by the federal government. It would share many principles with catastrophic coverage plans, whereby the cost of a list of drugs would be covered beyond a set threshold. This approach would provide public plans with financial support for Canadians with particularly high drug expenditures. Such an approach could target those with the highest need first, build on the existing funding for expensive drugs for rare diseases and develop the platform and infrastructure for a more comprehensive and co-ordinated approach to drug coverage across Canada.
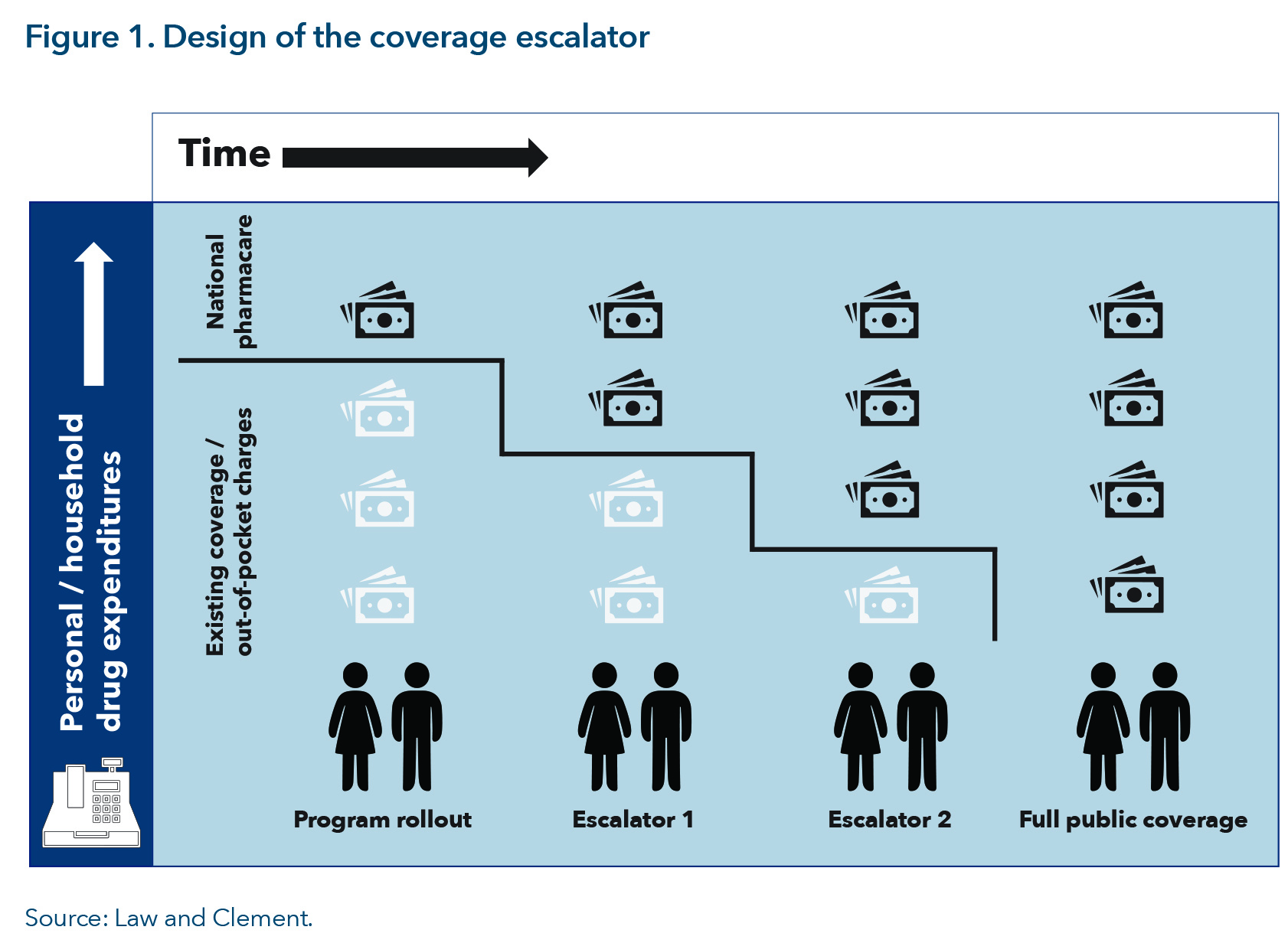
It would include the use of a defined national formulary, coupled with price negotiations at the national level for inclusion on the federal list. To align with the above principles, such a plan would need to cover the entire population but be designed at the outset to include generous coverage for low-income households. To achieve this, the plan should have two avenues for expansion: a coverage escalator to lower the reinsurance thresholds to achieve comprehensive public coverage, and a method to increase over time the formulary of drugs beyond those for rare diseases.
This model would include the following features:
With these features, the model would achieve the key principles stated above:
Along with achieving the above principles, this model would have several other positive impacts:
How much a federal reinsurance plan will cost depends on several key decisions made during its design. They include:
The development of a national formulary would be required for this plan to be enacted. To leverage the committed funding for expensive drugs for rare diseases, with perhaps some additional funding, the formulary would have to be a comparatively small list of high-cost medicines at the start. This list could be expanded over time to include more commonly used medications, while overlapping with public plan formularies to the maximum extent possible. This eventual overlap would be quite substantial in terms of the drugs that people use. For example, the Canadian Institute for Health Information, a research and advisory body funded by the federal, provincial and territorial governments, has estimated that drug classes found on 12 of the public drug program formularies constituted 89.9 per cent of all claims by seniors in 2016 (Canadian Institute for Health Information, 2016).
There is an empiric rationale to support an initial threshold around $60,000 of household income, as noted above. Alternatively, it could be set at $90,000, the same threshold used in the new federal dental benefit. The relationship between household income and cost-related non-adherence is reasonably linear up to approximately $100,000. Reductions in the threshold would result in proportionate declines in the amount of cost-related non-adherence that could be addressed (Law et al., 2018). Increases in the threshold through the escalator would expand the plan to cover more, and eventually all, Canadians.
The provinces and territories have public drug programs that cover a significant number of the medicines that would be included in a federal reinsurance plan. Its creation would offset some existing provincial and territorial spending and free up resources. Whether these offset amounts continued to be or are required to be spent on drug coverage will have important implications for the number of drugs that could be included on the formulary.
Consistent, comprehensive data will be required to support the implementation of this approach. This data collection would build upon the momentum already established by some large investments in robust pan-Canadian data, such as funding for the Health Data Research Network Canada. Its members include federal, provincial and territorial governments and organizations that have a national health mandate or hold national data. The network is helping standardize the data collected by provinces and territories (Health Data Research Network Canada, 2023). Universal capture of prescription drug use would have obvious benefits for managing the reinsurance plan. It would also enable research and evidence-informed decision-making about which drugs to cover.
We have existing public plans elsewhere in Canada that are similar to this approach. Yet cost-related non-adherence continues to persist. This raises the question of why the proposed approach might work at the federal level. We view our proposed plan as the thin end of the wedge. It capitalizes on the current context to lay the groundwork for national pharmacare. Importantly, our approach will bring the federal government to the table, outline its financial contributions and create a viable pathway to more comprehensive and co-ordinated universal coverage.
One common argument against national pharmacare is that it will not cover new and/or high-cost drugs. There is nothing inherent in this model, nor indeed the broader vision of comprehensive national pharmacare, that would preclude the listing of high-cost and newer medications. In fact, they would be included if the program started with the existing funding for expensive drugs for rare diseases. Formulary design at the national level would ensure a more consistent and fair application of rules across the country to determine what we should pay for, given a particular budget. Decisions about listing particular drugs could be driven by value (among other factors). The ultimate size of the formulary would depend on the level of funding provided to the program and how much of the cost is charged to patients. Finally, this plan would provide a backstop for the funding of many high-cost drugs, an increasing problem for small- and medium-sized employers with private benefits plans (Telus Health, 2023).
There would, of course, be a requirement to maintain and update the formulary. It requires significant human resources to assess drugs for addition to the list and to identify those that should be de-listed because of concerns about their safety, effectiveness or value. By consolidating the current formularies of public and private plans, the work of formulary management would also be consolidated, reducing duplication of work. This component builds on the momentum created by the establishment of the Canadian Drug Agency, whose role is to develop, maintain and update a national formulary.
Critics of this proposal may argue that drug purchasing will remain fragmented, diminishing possible bargaining power with pharmaceutical companies. However, the pan-Canadian Pharmaceutical Alliance already negotiates with pharmaceutical companies on behalf of all the public plans, seeking lower prices for Canadians. It is worth noting that, while complete consolidation of the sector to create a bargaining block may increase negotiating power, Canada remains a small component of the global market. Its influence is dwarfed by that of Europe and the United States. In addition, Canada has signalled through multiple other avenues, such as abandoning recently proposed changes to the Patented Medicine Prices Review Board, that the government has little appetite for new approaches in the current policy environment.
One concern with any stepped approach to national pharmacare is that the next steps will not be taken. In our model, the argument would translate to the coverage escalator not being implemented, leaving us with just a federal reinsurance system. There are two responses to this critique. First, the federal government could enshrine the escalator in any funding agreements signed with the provinces and territories. This would force future governments to honour this commitment. There would also be continued political pressure for additional support, as there is for the federal funding that contributes to physician and hospital services in provincial medicare programs. Second, even absent the coverage escalator, the reinsurance plan would improve access to expensive drugs for rare diseases and lay the groundwork for improved co-ordination of coverage in Canada.
We believe it is crucial to take a meaningful step toward national pharmacare and not lose this opportunity for progress. The approach laid out above would achieve the stated goals once it is fully in place. It would improve access to medicines, increase equity in the system and improve how drugs are prescribed and used. Importantly, it would be consistent with the implementation principles outlined above. It is the most practical approach that maintains universality as a core principle. This proposal advances coverage for those with the highest need, builds on existing momentum and will create a platform from which further progress could be made.
Acosta, A., Ciapponi, A., Aaserud, M., Vietto, V., Austvoll-Dahlgren, A., Kösters, J. P., Vacca, C., Machado, M., Diaz Ayala, D. H., & Oxman, A. D. (2014). Pharmaceutical policies: Effects of reference pricing, other pricing, and purchasing policies. Cochrane Database Systematic Reviews, 2014(10), Article CD005979. https://pubmed.ncbi.nlm.nih.gov/25318966/
Advisory Council on the Implementation of National Pharmacare. (2019). A prescription for Canada: Achieving pharmacare for all. Final report. Government of Canada.
https://publications.gc.ca/site/eng/9.873285/publication.html
Bolatova, T., & Law, M. R. (2019). Income-related disparities in private prescription drug coverage in Canada. CMAJ Open, 7(4) E618-623. https://www.cmajopen.ca/content/7/4/E618
Canadian Institute for Health Information. (2018). Drug use among seniors in Canada, 2016. Canadian Institute for Health Information.
https://secure.cihi.ca/free_products/drug-use-among-seniors-2016-en-web.pdf
Commission on the Future of Health Care in Canada. (2002). Building on values: The future of health care in Canada. Final report. Government of Canada.
https://publications.gc.ca/collections/Collection/CP32-85-2002E.pdf
Daw, J. R., & Morgan, S. G. (2012). Stitching the gaps in the Canadian public drug coverage patchwork? A review of provincial pharmacare policy changes from 2000 to 2010. Health Policy, 104(1), 19-26. https://pubmed.ncbi.nlm.nih.gov/21978939/
Government of Canada. (2019). Budget 2019: Moving forward on implementing national pharmacare. https://www.budget.canada.ca/2019/docs/themes/pharmacare-assurance-medicaments-en.html
Government of Canada. (2023). Budget 2023: A made-in-Canada plan. Strong middle class. Affordable economy. Healthy future. https://www.budget.canada.ca/2023/pdf/budget-2023-en.pdf
Health Canada. (2023). Investments to support access to drugs for rare diseases. [Backgrounder]. https://www.canada.ca/en/health-canada/news/2023/03/investments-to-support-access-to-drugs-for-rare-diseases.html
Health Data Research Network Canada. (2023). About HDRN Canada. [Web page].
https://www.hdrn.ca/en/about/
Holbrook, A. M., Wang, M., Lee, M., Chen, Z., Garcia, M., Nguyen, L., Ford, A., Manji, S., & Law, M. R. (2021). Cost-related medication nonadherence in Canada: A systematic review of prevalence, predictors, and clinical impact. Systematic reviews, 10(1), Article 11.
https://pubmed.ncbi.nlm.nih.gov/33407875/
IRPP Task Force on Health Policy. (2000). Recommendations to first ministers. IRPP.
https://irpp.org/research-studies/irpp-task-force-on-health-policy/
Law, M. R., Cheng, L., Kolhatkar, A., Goldsmith, L. J., Morgan, S. G., Holbrooke, A. M., & Dhalla, I. A. (2018). The Consequences of patient charges for prescription drugs in Canada: A cross-sectional survey. CMAJ Open, 6(1) E63-E70. https://www.cmajopen.ca/content/6/1/E63
Liberal Party of Canada and the New Democratic Party. (2022). Delivering for Canadians now, A supply and confidence agreement. Prime Minister of Canada.
https://www.pm.gc.ca/en/news/news-releases/2022/03/22/delivering-canadians-now
National Forum on Health. (1997). Canada health action: Building on the legacy. Final report Volume 1. Government of Canada.
https://www.canada.ca/en/health-canada/services/health-care-system/reports-publications/health-care-renewal/canada-health-action-building-legacy-volume1.html
Office of the Parliamentary Budget Officer. (2023). Cost estimate of a single-payer universal drug Plan. Government of Canada. https://www.pbo-dpb.ca/en/publications/RP-2324-016-S–cost-estimate-single-payer-universal-drug-plan–estimation-couts-un-regime-assurance-medicaments-universel-payeur-unique
Patented Medicine Prices Review Board. (2017). Alignment among public formularies in Canada. Part 1: General Overview. Government of Canada. http://www.pmprb-cepmb.gc.ca/view.asp?ccid=1327
Royal Commission on Health Services. (1964). Final report. Volume 1. Government of Canada. https://publications.gc.ca/site/eng/9.818794/publication.html
Telus Health. (2023). 2023 Drug data trends & national benchmarks. Telus Health.
https://healthlibrary.telus.com/en/insurers/your-copy-awaits-the-2023-drug-data-trends-national-benchmarks-report
World Health Organization. (2021). WHO model list of essential medicines – 22nd list, 2021. World Health Organization. https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2021.02
This insight was published as part of the Toward a More Equitable Canada research program, under the direction of Shaimaa Yassin. The manuscript was copy-edited by Madelaine Drohan, proofreading was by Zofia Laubitz, editorial co-ordination was by Étienne Tremblay, production was by Chantal Létourneau and art direction was by Anne Tremblay.
Michael Law is a professor and Canada Research Chair in Access to Medicines at the University of British Columbia.
Fiona Clement is a professor and department head at the University of Calgary.
To cite this document:
Law, M., and Clement, F. (2024). National pharmacare: Laying the groundwork. IRPP Insight No. 51. Montreal: Institute for Research on Public Policy.
The opinions expressed in this paper are those of the authors and do not necessarily reflect the views of the IRPP, its Board of Directors, or sponsors. Research independence is one of the IRPP’s core values, and the IRPP maintains editorial control over all publications.
IRPP Insight is a refereed series that is published irregularly throughout the year. It provides commentary on timely topics in public policy by experts in the field. Each publication is subject to rigorous internal and external peer review for academic soundness and policy relevance.
If you have questions about our publications, please contact irpp@nullirpp.org. If you would like to subscribe to our newsletter, IRPP News, please go to our website, at irpp.org.
Illustration: Shutterstock.com
ISSN 2291-7748 (Online)